1. WHY SCOTLAND MUST CHANGE
A Note on Tone This opening section focuses deliberately on the scale and nature of Scotland's challenges. It strikes a more sombre tone than other parts of this report. This is intentional: a clear understanding of the pressures facing Scotland's people, services, and finances is essential groundwork for the solutions that follow. The subsequent sections of Part 2 — and the A.R.I.S.E. Blueprint in Part 1 — set out a practical, achievable and evidence-based pathway for meeting these challenges and building a positive future.
A Nation at a Crossroads
Scotland stands at a defining moment. After decades of progress in public health and social policy, we face a convergence of challenges that demand transformational thinking. This is not a story of inevitable decline — but neither is it a story where transformation will be quick or simple. In this Section we set out why Scotland must change, and why this change is urgent; it is followed by more optimistic sections showing how change can succeed, and how it may be funded from existing resources. The leaders reading this report have repeatedly demonstrated remarkable capacity for innovation. From the rapid transformation during COVID-19 to pioneering approaches to prevention in places like Clackmannanshire, Dundee, Glasgow, Lanarkshire, and the Lothians (with apologies to the many we have missed), Scotland's public service executives possess the strategic vision and operational expertise needed for the changes ahead. Yet the scale of change required will test this capacity to its limits. The question is not whether Scotland has the capability to transform — it is whether we can sustain the political will, resource allocation, and cultural change necessary for comprehensive success over the long term.
The Foundation for Change
Policy Alignment Creates Unprecedented Opportunity
Scotland's 2025 Population Health Framework (Scottish Government, 2025a) commits to "shift from reactive spending to preventative investment" and "developing new resource allocation approaches that support prevention." This aligns with the 2025 Public Sector Reform Strategy's call (Scottish Government, 2025b) for moving from reactive to preventative spending, the Health and Social Care Service Renewal Framework's acknowledgment that system pressures cannot be resolved without upstream prevention, and the United Nations Convention on the Rights of the Child (UNCRC) incorporation (Scottish Parliament, 2024) which creates binding legal obligations to prioritise children's wellbeing and protection from harm. Yet the Population Health Framework acknowledges the scale of challenge, noting "financial pressures across the public sector" and recognising the need for "practical architecture" to turn these commitments into operational reality. This Commission's A.R.I.S.E. Blueprint provides exactly this architecture — the implementation manual Scotland's prevention agenda requires.
Scotland's Innovation Track Record
Before examining current challenges, it is crucial to recognise what Scotland's public service leaders have already achieved. The Early Years Collaborative (Scottish Government, 2012), evolving into the Children and Young People Improvement Collaborative (CYPIC) (Scottish Government, 2016), demonstrated how health, education, and local government can collaborate effectively. Local innovations documented during our inquiry include whole systems approaches to children and families, integrated family support teams, creative use of change funds to reallocate spending from reactive adult services to preventive early-years initiatives, and community-based prevention approaches to tackle adverse childhood experiences (ACEs). Other successes include the Universal Health Visiting Pathway (Public Health Scotland, 2021), increasing health visitor numbers (while they reduced in England), Family Nurse Partnership (NHS Health Scotland, 2019), and initiatives supporting Perinatal Mental Health. The rapid COVID-19 response provided further proof of Scottish leaders' innovation and adaptability. Yet fourteen years after Christie (Christie Commission, 2011), the scale of problems below suggests that creative local innovation — however impressive — is insufficient without systematic change across Scotland's public services.
1.1 The Current Crisis: Unsustainable System
Pressures The Convergence of Multiple Crises
Local authorities and NHS Boards face an unprecedented convergence of financial, demographic, operational, and political pressures. The Population Health Framework acknowledges that "unless we make this shift to prevention, the demands on support and services will only increase."
Local Authorities: Eight Critical Challenges
1. Unsustainable Service Demand: Rising demand for social care, homelessness support, and mental health interventions while capacity declines. Child protection referrals and social care caseloads have grown significantly, with efficiency gains "outstripped by demand."
2. Workforce Crisis: Critical posts across education, planning, social work, and finance remain unfilled. One CEO noted "sustained vacancies in skilled roles are eroding the ability to deliver statutory services."
3. Child Poverty Mandate vs. Limited Levers: Legal accountability for eradicating child poverty by 2030, yet councils frequently lack levers to impact key drivers like housing supply, social security, or labour markets.
4. The Promise Implementation Gap: Commitment to delivering "The Promise" (Independent Care Review, 2020) faces mismatches between ambition and resources, particularly for shifting from residential to community-based care. The Promise's vision aligns perfectly with prevention approaches: both recognise that supporting families before crisis prevents the need for care placements.
5. Multiple Competing Priorities: Councils must deliver on reducing poverty, transitioning to net zero, supporting sustainable public services, and improving outcomes for children — all with limited resources.
6. The Reactive Spending Trap: Short-term cuts to meet statutory obligations, but known to harm longer-term outcomes — reductions in early intervention 2 services, youth provision, public health budgets — the trap England followed in the 2010s with the consequences outlined by five major children's charities in 'The Long Road to Recovery' (Larkham & Ren, 2025): Rise in children entering care, increases in child poverty and homelessness, sharp deterioration in child mental health and increased later, high-cost interventions.
7. Political Decision-Making Constraints: Short-termism, political churn, and populist pressures hinder strategic decisions, with frequent reversals of long term plans following elections.
8. Capital Investment Backlogs: Ageing infrastructure deteriorates while budget constraints defer maintenance and cancel upgrades. CEOs warn of long-term service degradation and safety risks.
NHS Boards: Five Critical Pressures
1. Workforce Shortages and Burnout: High vacancy rates across clinical professions, with existing staff facing growing burnout while Boards rely on costly agency workers.
2. Financial Unsustainability: Structural deficits, non-recurring funding reliance, and falling capital investment, with multiple Boards reporting they cannot meet demand, maintain safety, and deliver savings simultaneously.
3. Treatment Target Dilemma: Growing tension between political expectations to reduce waiting times and Boards' capacity constraints within budget and workforce limits.
4. Mental Health and Addiction Demand: Rising demand outstrips funding and staff, with many cases reflecting deeper socio-economic drivers that leave Boards trying to solve problems they did not create.
5. Performance Pressure Without System Change: Boards report being "bombarded" with performance frameworks, inspections, and improvement plans that can be duplicative, inconsistent, and distract from operational delivery.
Shared Systemic Issues
Complex responsibilities across health, social care, education, justice, and third sector make coordination difficult; national plans often lack practical delivery support; annual budgeting undermines transformation efforts; and growing gaps exist between citizen expectations and available resources. These challenges reflect system design that was fit for purpose in a different era but is now fundamentally misaligned with the demographic, fiscal, and social realities of the 2020s.
1.2 The Scale of Preventable Harm: Scotland's £6 Billion Crisis
The Evidence Base for Primary Prevention
Scotland's fiscal and operational crisis is largely a consequence of decades of underinvestment in early, upstream intervention. The Population Health Framework explicitly recognises that "primary prevention is 3–4 times more cost-effective than investing in treatment."
The ACEs Reality3 Along with Wales, Scotland has led the UK in recognising the powerful negative impact of ACEs. The 2019 Scottish Health Survey (Scottish Government, 2020) revealed: • 71% of adults had experienced at least one ACE • 15% reported four or more ACEs • The most prevalent were verbal abuse (47%), physical abuse (28%), domestic violence (24%), parental separation (23%), household mental illness (19%), and household alcohol abuse (16%)
The Devastating Impact of Multiple ACEs
Evidence from Welsh ACE studies shows people with four ACEs face dramatically higher risks than those with none (Bellis et al., 2015):
• 3 times higher risk of heart disease, respiratory disease, and type 2 diabetes
• 4 times higher risk of being a high-risk drinke
r • 5 times higher risk of having low mental wellbeing
• 15 times higher risk of committing violence
• 16 times higher risk of using crack cocaine or heroin
• 20 times higher risk of imprisonment
The £6 Billion Annual Cost
Using the 2.8% of UK GDP rate for ACE-related costs calculated by Hughes et al. (2021), Scotland faces an annual burden exceeding £6 billion — over £90 million per local authority and almost £220 million per Territorial NHS Board annually. This covers only ACE-related harm; including other preventable difficulties like insecure attachment and Foetal Alcohol Spectrum Disorders substantially increases the huge scale of Scotland’s preventable costs.
The Human Reality
Evidence from survivors includes: "My mother screaming at me, calling me names, and putting me down. When [spanking me] she would be so angry that she would lose control." "My earliest childhood memory is me sitting alone in my room staring at a wall and hugging my teddy." "Over the next eight years, I endured sexual abuse more times than I could count. I lived in fear." For survivors, these problems often persist to adulthood: "My experiences of being neglected as a child are with me every day ... It was just hell" "I have been in and out of therapy for 25 years... Every day is a struggle with self-esteem." One NSPCC survey (NSPCC, 2023) found 18.6% of UK secondary school children had been severely abused or neglected. Applied to Scotland, this could fill Hampden Park more than 19 times over.
The Primary Prevention Opportunity: Evidence of What Works
Alongside targeted, evidence-based programmes, Scotland has already shown that large-scale, system-wide action can deliver meaningful gains. These include increases in health visitor numbers, strengthened perinatal mental health provision, reductions in children entering care in Glasgow, and North Lanarkshire's notable rise in breastfeeding uptake and duration.4 At the programme level, there is clear evidence that well-timed early-years interventions such as Parent-Child Psychological Support (PCPS), Mellow Parenting (Raouna et al., 2021) and perinatal support services can achieve both short- and long-term improvements. Within two years, interventions like PCPS show significant reductions in insecure attachment and children taken into care, alongside improved parental sensitivity, sense of parental competence, and reduced parental stress (Bujia-Couso et al., 2010). Within four years, primary prevention approaches will demonstrate better child executive function, self-control, emotional regulation, and school readiness. Later in this report, we will demonstrate how the absence of these four skills in children generates enormous annual costs in fields such as academic achievement, antisocial behaviour, benefit dependency, crime, domestic abuse, mental health, persistent unemployment, school behaviour, and tax revenue. The significant cost savings from this core change in focus will stretch over future decades and generations.
Scotland's Third Sector: Essential Partners in Transformation Scotland is extraordinarily fortunate to possess many excellent third sector organisations who carry out work of exceptional value in supporting children and families. From national organisations like Barnardo's Scotland, Children in Scotland, Children 1st, and NSPCC Scotland, to local community groups providing direct support, these organisations possess irreplaceable expertise, community trust, and innovative approaches that will be absolutely vital to successful transformation. Their current funding falls well short of what their contribution merits, and any serious prevention strategy must recognise that these organisations are not additional extras but core partners whose expanded role will be essential for reaching families and delivering prevention support at the scale required. We believe that local authorities and NHS Boards in the UK, including Scotland, spend less than 2% of their budgets on primary prevention – preventing harm before it happens. We recently asked Grok AI to estimate how much Scotland’s statutory agencies spend on developmental primary prevention – i.e. excluding immunisations and only addressing prevention affecting the social and emotional health and welfare of children. Its estimate was less than 0.5% of budgets.
1. Reallocation of resources to developmental primary prevention The Commission of Inquiry recommends reallocating 4–6% of statutory budgets over time to developmental primary prevention. A shift on this scale is required to enable the transformation of Scotland’s health, wealth and social conditions that the Commission believes is possible. The A.R.I.S.E. Blueprint sets out a practical, evidence-based approach to identifying and releasing the resources required to support this reallocation.
1.3 Scotland: A Nation Living Beyond its Means
The Fiscal Outlook: A Path That Cannot Continue
The fiscal deficit in Scotland of £22.7 billion in 2023–24 (10.4% of GDP) was more than double the UK average of 4.5%. Scotland confronts what the Auditor General has termed an "unsustainable financial position." The Scottish Fiscal Commission's 5 April 2025 Fiscal Sustainability Report (Scottish Fiscal Commission, 2025) shows that Scotland's structural deficit — the gap between spending and revenue — persists even during economic stability. Health and social care costs are rising faster than economic growth, while the proportion of working-age taxpayers is falling. The Scottish Government's 2025 Medium-Term Financial Strategy (Scottish Government, 2025c) forecasts that day-to-day funding pressures could exceed resources by £1– 1.9 billion annually by 2027–28. The longer local authorities and NHS Boards defer action, the deeper Scotland moves into a future in which ever-larger portions of the budget are consumed by reactive spending, making necessary change progressively harder to implement. Taken together, Scotland's fiscal reality and the Population Health Framework's call for a decisive shift from reactive to preventative investment create an overwhelming case for immediate action.
Demographic Pressures Scotland's population is ageing rapidly. Over-65s will grow by nearly a third by 2045, and those aged 75+ by 25% in the next decade, while the working-age population shrinks. Without systematic change, health and social care spending could rise from 50% to over 60% of devolved expenditure by 2035 — crowding out investment in education, housing, and infrastructure.
Healthcare Crisis Despite a 21% real terms rise in direct health spending between 2013–2014 and 2022–2023, outcomes are worsening. Key indicators reveal the strain: staff sickness reached 6.2% in 2022–2023 — the highest in a decade. Most waiting standards aren't met. Delayed discharges cost over £200 million per year. Boards must deliver 6% efficiency savings in 2024–2025 — well beyond historical norms. Recent audit reports reinforce these concerns. A sample of just three NHS Boards showed: one with a £46.5 million funding gap requiring extensive reliance on non recurring savings; one requiring £28.4 million in bailouts to break even; and a third facing recurring deficits and needing over £200 million in savings over three years.
Local Government Strain
While Scottish Government revenue funding rose in cash terms between 2013–2014 and 2023–2024, real-terms value fell, especially in general revenue grants — the part councils control. Cuts have hit unprotected services hardest: Environmental services: down 30%, Culture and leisure: down 25%, Planning: down 40%. Meanwhile, demand is rising in housing, education, and mental health, with escalating costs of temporary accommodation and children in care. COSLA estimates a £1 billion funding gap in 2023–2024. Two-thirds of councils used reserves to fill deficits. Audit Scotland concluded in its Local Government in Scotland - Overview 2023 (Accounts Commission, 2023): "Radical change is urgently needed if councils are to maintain services," and "Reform should prioritise prevention."
Three Strategic Choices
Option 1: Continue as Present — Leads to inevitable service collapse as evidence confirms Scotland's local areas cannot meet legal and policy commitments under the current model.
Option 2: Proceed Slowly — Gradual change risks being overtaken by accelerating demographic and fiscal pressures.
Option 3: Embrace Transformative Prevention — Strategic reallocation to proven primary prevention can reduce long-term costs while improving outcomes, though requiring sustained commitment over multiple years.
The Legal Imperative The United Nations Convention on the Rights of the Child (UNCRC) — incorporated into Scots law in 2024 — creates binding obligations requiring public bodies to ensure children's rights to health, education, and protection from harm. It could be argued that allowing children to develop insecure attachment, or harmful ACEs, while there are known, cost-effective methods to protect children from these, constitutes a breach of those rights. Continued underinvestment in primary prevention risks breaching children's rights systematically while deepening fiscal crisis.
1.4 Why This Time Will Be Different: Learning from Christie The 2011 Christie Commission called for prevention and early intervention, yet transformation remained partial. Five factors now distinguish this moment:
1. Fiscal Imperative Creates Political Will: Previously, leaders could choose between prevention and maintaining existing services. Now crisis services themselves are failing, making transformation necessary rather than optional.
2. Legal Obligations Provide Foundation: UNCRC obligations create enforceable duties that cannot be easily ignored, making primary prevention legally necessary.
3. Implementation Guidance Exists: Where Christie provided limited operational detail, this Commission offers specific interventions, resource reallocation mechanisms, and implementation processes from successful examples.
4. Policy Infrastructure Aligned: Multiple government strategies now point toward similar transformation goals, creating a coherent foundation for systematic change.
5. Recognition That Prevention Requires Cultural as Well as Structural Change: Previous reform efforts focused primarily on reorganising services and reallocating budgets without addressing why demand for reactive interventions persists.
2. Community and statutory co-responsibility for prevention The Commission of Inquiry recommends that prevention strategies in Scotland are designed on the basis that sustainable prevention requires both system redesign and intentional shifts in how communities support families and share responsibility for children’s wellbeing and outcomes.
International Precedent: Proven Universal Early Years Models from the Netherlands, Denmark and Sweden For more than two decades the Netherlands, Denmark and Sweden have consistently occupied the top tier of UNICEF Innocenti child well-being rankings (UNICEF, 2025) among rich countries. Each offers a complementary, evidence based component that together forms a complete blueprint for transformative early years reform in Scotland.
• The Netherlands (ranked 1st in every UNICEF league table since 2007) demonstrates the decisive impact of intensive, health-led primary prevention from day one. Automatic enrolment into Kraamzorg (8–10 days of skilled in home postnatal care) and Consultatiebureaus (a nationwide network of free child health clinics reaching ~95% of 0–4-year-olds) detects issues early, builds parental capability and generates estimated returns of €2–3 for every €1 invested (RIVM, 2023).
• Denmark (2nd in both the 2020 and 2025 UNICEF Report Cards) shows how a fully universal, high-quality early childhood education and care system from six months of age sustains outstanding mental, physical and social outcomes even through crises such as COVID-19. Near-universal enrolment (90–96%), capped parent fees, strong staff-to-child ratios and a play-based social pedagogy curriculum deliver returns of €2–3 per €1 invested while keeping child life-satisfaction and health among the highest in the world.
• Sweden complements the other two with its integrated "educare" model and generous parental leave framework. Subsidised, play-based preschool for virtually all children from age 1, combined with 480 days of well-paid leave, has driven female employment to 82%, reduced later mental-health diagnoses and produced long-term fiscal returns of €2.50–€3.00 per €1 spent (OECD, 2024; Skolverket, 2023). The economic case for these systems is compelling, with quantifiable cost-benefit evidence underscoring their efficiency in reducing later interventions, enhancing equity and boosting productivity. The table below summarises key metrics, drawing on national evaluations and OECD benchmarks.
Outcome area Preventive health & acute care Maternal workforce participation Netherlands evidence (2022– 2024) €2–3 saved per €1 invested; 20–30 % reduction in preventable hospital admissions (Ministry of Health/RIVM) Kraamzorg enables 85 % return-to-work Denmark evidence (2022– 2024) €2–3 saved per €1 invested; 15– 25 % drop in later mental-health needs via universal ECEC (Danish Health Authority) Universal ECEC lifts female employment to Sweden evidence (2021–2024) €1.2 bn annual national savings from high immunisation coverage; €1 500– 2 000 per child in avoided mental health treatment Universal preschool → 82 % female Indicative long-term ROI 2–3 : 1 3–4 : 1
Outcome area Equity & lifetime social costs Netherlands evidence (2022– 2024) within 6 months → €4–5 bn annual GDP gain (CBS, 2024) 95 % participation narrows socio economic health gaps by ~25 %, averting ≈ €800 m in lifetime costs (RIVM, 2022) Denmark evidence (2022– 2024) ~80 % → €3–4 bn annual GDP contribution (Statistics Denmark, 2024) 90–96 % enrolment equalises outcomes, saving ~€2 bn in inequality-related costs since 1990s (Danish Ministry of Education) Sweden evidence (2021–2024) employment rate → €10–12 bn annual GDP contribution (OECD, 2024) Expansion 1970– 1998 equalised outcomes and saved ≈ €3 bn in inequality-related interventions (Skolverket, 2023) Indicative long-term ROI 2.5–3 : 1
Taken together, these three small nations illustrate that a coherent, universal early years system — combining intensive postnatal support (Netherlands), seamless high-quality educare from infancy (Denmark) and strong family-workforce policies (Sweden) — is not only feasible but politically durable when protected by cross-party consensus and stable investment of 1–1.5% of GDP. For Scotland, adopting these proven elements offers a realistic pathway to move the United Kingdom out of the lower half of international child well-being tables within a decade, while delivering health, equity and productivity gains conservatively estimated at tens of £billions over ten years. The evidence is clear: sustained political commitment to universal prevention, as demonstrated by these three countries, transforms child outcomes and pays for itself many times over.
An Appeal to Scotland's Political Leaders When this Commission of Inquiry was launched in 2022, every party leader in the Scottish Parliament had pledged support for the 70/30 objective: to reduce levels of child abuse, neglect, and children witnessing domestic violence by 70% by 2030. The Commission, under the leadership of Sir Harry Burns, was challenged to design a feasible action plan to deliver that result. We believe the 'Transforming Scotland in a Generation' A.R.I.S.E. Blueprint will deliver that for future generations of Scotland's children — and transform the life chances of Scotland's children. As Scotland approaches its next General Election, the temptation to score media and publicity points over political opponents will be very strong. We pray that, in this realm at least, cross-party support will continue and prevail. The Netherlands and Scandinavian lessons are unmistakable: lasting transformation comes only when political leaders sustain common commitment across successive governments.
1.5 Scotland's Transformation Opportunity
The Alignment of Conditions
The convergence of fiscal crisis, legal obligations, policy alignment, and implementation guidance creates Scotland's best opportunity for systematic change. The Population Health Framework provides policy commitment; this Commission's Blueprint provides operational detail; fiscal pressures create political urgency; UNCRC obligations provide legal imperative.
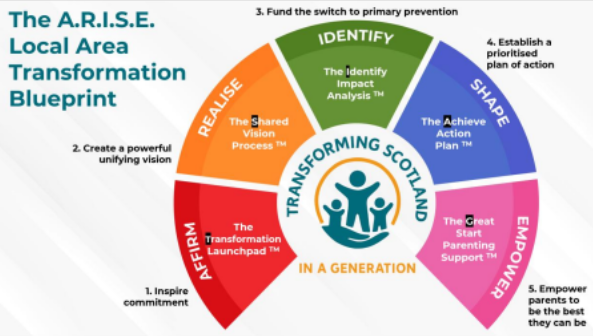
The Implementation Pathway Success requires:
• Commitment: Building sustained political support across electoral cycles
• Vision: Creating shared understanding across sectors
• Evaluation: Implementing resource reallocation approaches using evidence based guidance
• Prioritised Action: Deploying interventions proven most effective while adapting to local circumstances
• Empowering Parents: Using Scotland's universal health visiting infrastructure and other means, discussed in this report, to deliver foundational support
Scotland's Choice Scotland's leaders can continue managing decline through reactive spending that grows more expensive while struggling to meet legal obligations to children, or they can seize this opportunity to begin building effective public services focused on prevention and early intervention. The elements for transformation are now aligned. Scotland has demonstrated capacity for innovation repeatedly — from the Early Years Collaborative to COVID 19 adaptation. The opportunity exists to channel that proven capability toward systematic primary prevention.
This is Scotland's opportunity to take a giant leap toward becoming the best place in the world for children to flourish.
References
Accounts Commission. (2023). Local government in Scotland: Overview 2023. Audit Scotland. https://www.audit-scotland.gov.uk/publications/local-government-in scotland-overview-2023 Bellis, M. A., Lowey, H., Leckenby, N., Hughes, K., & Harrison, D. (2015). Adverse childhood experiences: Retrospective study to determine their impact on adult health behaviours and health outcomes in a UK population. Journal of Public Health, 36(1), 81–91. https://doi.org/10.1093/pubmed/fdt038 Bujia-Couso, P., O'Rourke, A., & Cerezo, M. A. (2010). Criteria based case review: The Parent Child Psychological Support Program. Irish Journal of Applied Social Studies, 10(1), Article 1. https://doi.org/10.21427/D7Z722 Christie Commission. (2011). Commission on the future delivery of public services. Scottish Government. https://www.gov.scot/publications/commission-future-delivery public-services/ Hughes, K., Ford, K., Bellis, M. A., Glendinning, F., Harrison, E., & Passmore, J. (2021). Health and financial costs of adverse childhood experiences in 28 European countries: A systematic review and meta-analysis. The Lancet Public Health, 6(11), e848–e857. https://doi.org/10.1016/S2468-2667(21)00232-4 Independent Care Review. (2020). The Promise. Independent Care Review. https://www.carereview.scot/destination/promise/ Larkham, J., & Ren, A. (2025). A long road to recovery: Local authority spending on early intervention children's services 2010/11 to 2023/24. Children's Charities Coalition, London. https://www.childrenscharitiescoalition.org.uk/reports/long-road recovery NHS Health Scotland. (2019). Revaluation of Family Nurse Partnership in Scotland: Qualitative study. NHS Health Scotland. https://www.healthscotland.scot/publications/revaluation-of-family-nurse-partnership in-scotland-qualitative-study NSPCC. (2023). Statistics on child abuse. NSPCC. https://learning.nspcc.org.uk/statistics-child-abuse/ OECD. (2024). Education at a glance 2024: OECD indicators. OECD Publishing. https://doi.org/10.1787/e13bef63-en Public Health Scotland. (2021). Evaluation of the Universal Health Visiting Pathway in Scotland: Phase 1 report. Public Health Scotland. https://publichealthscotland.scot/publications/evaluation-of-the-universal-health visiting-pathway-in-scotland-phase-1-report-primary-research-with-health-visitors and-parents-and-case-note-review/ Raouna, A., Malcolm, R., Ibrahim, R., & MacBeth, A. (2021). Promoting sensitive parenting in 'at-risk' mothers and fathers: A UK outcome study of Mellow Babies, a group-based early intervention program for parents and their babies. PLOS ONE, 16(2), e0245226. https://doi.org/10.1371/journal.pone.0245226 RIVM. (2023). Monitor Kansrijke Start 2023. National Institute for Public Health and the Environment. https://www.rivm.nl/monitor-kansrijke-start-202311 Scottish Fiscal Commission. (2025). Fiscal sustainability report (April 2025). Scottish Fiscal Commission. https://www.fiscalcommission.scot/publications/fiscal sustainability-report-april-2025/ Scottish Government. (2012). Early Years Collaborative. Scottish Government. https://www.gov.scot/policies/improving-public-services/early-years-collaborative/ Scottish Government. (2016). Children and Young People Improvement Collaborative. Scottish Government. https://www.gov.scot/policies/improving-public services/children-and-young-people-improvement-collaborative/ Scottish Government. (2020). Scottish Health Survey 2019. Scottish Government. https://www.gov.scot/publications/scottish-health-survey-2019-volume-1-main-report/ Scottish Government. (2025a). Scotland's Population Health Framework 2025-2035. Scottish Government. https://www.gov.scot/publications/scotlands-population-health framework-2025-2035/ Scottish Government. (2025b). Scotland's Public Service Reform Strategy – Delivering for Scotland. Scottish Government. https://www.gov.scot/publications/scotlands-public-service-reform-strategy delivering-scotland/ Scottish Government. (2025c). Scotland's fiscal outlook: Medium-term financial strategy (June 2025). Scottish Government. https://www.gov.scot/publications/scotlands-fiscal-outlook-scottish-governments medium-term-financial-strategy/ Scottish Parliament. (2024). United Nations Convention on the Rights of the Child (Incorporation) (Scotland) Act 2024. Scottish Parliament. https://www.legislation.gov.uk/asp/2024/1/contents Skolverket. (2023). PISA 2022: 15-åringars kunskaper i matematik, läsförståelse och naturvetenskap. Swedish National Agency for Education. https://www.skolverket.se/publikationer?id=3706 UNICEF. (2025). Innocenti Report Card 19: Child well-being in an unpredictable world. UNICEF Office of Research – Innocenti. https://www.unicef irc.org/publications/series/report-card
Taken together, this evidence demonstrates that ACEs do not merely coexist with poor educational outcomes; they actively undermine the biological and psychological foundations upon which learning depends. Educational underachievement associated altered neurodevelopment driven by chronic stress exposure. with adversity is therefore not primarily a matter of motivation or capability, but of 9 Box X: How Adverse Childhood Experiences Disrupt Learning and School Success Synthesised from Nadine Burke Harris, Roadmap for Resilience: The California Surgeon General’s Report on Adverse Childhood Experiences, Toxic Stress, and Health (2020) Research synthesised in the California Surgeon General’s Roadmap for Resilience provides one of the most comprehensive accounts of how ACEs and toxic stress impair educational functioning. Key mechanisms and outcomes include: • Neurobiological disruption: Chronic activation of the stress response alters development of the amygdala, hippocampus, and prefrontal cortex—regions essential for memory, learning, emotional regulation, and executive function. • Impaired executive functioning: Toxic stress compromises impulse control, attention, working memory, and planning, making classroom learning and behavioural regulation significantly more difficult. • Reduced school engagement: Children with high ACE exposure are more likely to disengage from school, struggle with homework completion, and experience chronic absenteeism. • Learning and behavioural difficulties: ACE exposure is strongly associated with learning disabilities, behavioural dysregulation, and increased need for special education services. • Dose–response effects: The likelihood and severity of educational difficulties increase sharply with the number of ACEs experienced. • Scale of impact: Evidence indicates that over half of children with four or more ACEs experience learning or behavioural problems, compared with a very small minority of children with none. The Roadmap for Resilience emphasises that these outcomes are not inevitable. When toxic stress is prevented or buffered through safe, stable, and nurturing relationships, many of these neurobiological and educational harms can be mitigated or avoided altogether. Source: Bhushan et al., 2020. International Evidence. This dose-response relationship is replicated globally. A 2021 meta-analysis of 28 European countries estimated ACE-attributable costs between 1.1% and 6.0% of GDP, with violence, alcohol misuse, and mental illness carrying the highest burden (Hughes et al., 2021).10 Implications for Scotland. Preventing multiple ACEs would yield transformative benefits, reducing demand across health, justice, and social care while improving productivity and wellbeing. 12.7 The ACE Burden in Scotland Scotland’s 71% prevalence of at least one ACE underscores how widespread adversity is. This is not a marginal issue affecting only the most deprived: it is a population-wide challenge. The 15% reporting 4 or more ACEs face dramatically elevated risks across almost every health and social outcome. Distribution Across Society. While ACEs are more concentrated in deprived areas, they occur across all socioeconomic groups. Prevention must therefore be universal, but with proportionate intensity in areas of higher adversity. Hidden Burden of Neglect. As noted above, the Scottish Health Survey (2019) did not measure neglect, despite it being the most common form of maltreatment recorded by child protection systems. Scotland’s true adversity burden is therefore even higher than measured by the survey. Neglect is often chronic, invisible, and strongly associated with poverty, but also occurs – especially emotional neglect - across all communities. Economic Costs. Applying Hughes’UK GDP calculation (2.8%) to Scotland indicates an annual ACE-related burden of over £6 billion. Given Scotland’s higher prevalence rates, the true figure may be higher still. These costs manifest in NHS treatment, mental health, substance misuse services, criminal justice, social care, and lost economic output. Linking ACEs to System Pressures. ACEs underpin many of Scotland’s costliest challenges: violence, addiction, poor mental health, school exclusion, unemployment, and chronic disease. They are a prime "hidden source of dysfunction", intertwined with deficits in the four foundational skills dealt with in Section xxx, that explain why Scotland’s services are overwhelmed. Implications for Scotland. Reducing ACEs is both a moral and fiscal imperative. Without decisive action on prevention, Scotland’s public services will remain locked in unsustainable cycles of reactive spending. 12.8 Recommendations for Action Scotland has acknowledged ACEs through survey data and policy initiatives and has committed to greater priority for prevention through the Public Sector Reform Strategy (2025) and Population Health Framework (2025). These commitments provide a foundation on which to build. The earlier Section on Oral Evidence and Formal Written Submissions contains the Commission's overarching recommendation on ACE prevention:11 The Commission recommends that Scotland shift decisively from a predominantly trauma-response model to a trauma-prevention model, systematically addressing the family and relational conditions that generate ACEs. Rationale: Both oral and written evidence were unequivocal that maltreatment and ACEs are the most important preventable causes of later psychopathology and system demand. This section proposes enabling steps to underpin that shift. The roots of dysfunctional parenting are already addressed in earlier sections on promoting universal parenting support, supporting parental mental health, and prioritising parental sensitivity and secure attachment. Prevention of child sexual abuse is addressed in Section 13, and domestic abuse and violence in Section X. Here we address five additional enabling actions: (A) recognising and healing prior generation trauma; (B) addressing parental substance abuse; (C) educating the public about ACEs and related science; (D) strengthening professional recognition of ACEs; and (E) adopting a whole-system public health approach. (A) Recognising and Healing Prior Generation Trauma Prior generation trauma—parental histories of abuse, neglect, or significant loss in childhood—substantially elevates risks to child development by disrupting the capacity for secure attachment and sensitive caregiving. Serious case reviews in England have highlighted that parental childhood maltreatment often leads to underestimated vulnerabilities, contributing to infant harm through impaired emotional availability (Ofsted, 2011). Longitudinal studies confirm that parental childhood adversity predicts poorer outcomes in their own children, perpetuating cycles across generations (Plant et al., 2017). The primary mechanism is straightforward: most people parent the way they were parented, and without intervention, dysfunctional patterns are transmitted through modelling and relational experience. Breaking this cycle requires creating safe opportunities for parents to address their own histories. Trauma-informed approaches—including attachment-focused programmes, somatic therapies, and peer-led recovery groups—can help heal parental trauma and enhance capacity for sensitive caregiving. Where routine inquiry about childhood experiences is conducted within antenatal and perinatal services, this would be most effective when practitioners are trained in trauma-informed responses and appropriate support is readily available. Family hubs offer a promising setting for integrating such support with parenting education, counselling, and intergenerational family work. (B) Addressing Parental Substance Abuse12 Parental substance misuse—including alcohol, drug dependence, and smoking— profoundly undermines child development by disrupting secure attachment and impairing parental responsiveness to infants' cues. The consequences include neglect, emotional unavailability, chaotic home environments, and unmet safety and health needs, resulting in insecure attachments and long-term vulnerabilities (Hosking & Walsh, 2013). Prenatal exposure carries additional risks including miscarriage, low birth weight, and foetal alcohol spectrum disorders (FASD), with lifelong cognitive and behavioural impacts. Research confirms dose-response effects: higher maternal substance use correlates with significantly increased odds of child maltreatment (Freisthler et al., 2021). Effective prevention requires timely, stigma-free access to treatment for parents, integrated with whole-family support. Antenatal services offer a critical window for identification and early intervention. Peer recovery programmes and family-based interventions can support sustained change while protecting children's developmental needs. Training for health visitors and other practitioners in early identification and compassionate referral would strengthen the system's capacity to intervene before harm occurs. While compassionate support for parents with addiction is essential, the Commission notes that the UN Convention on the Rights of the Child places the child's safety and wellbeing at the centre of all decisions. Where parental substance misuse poses a risk to children, their protection must take priority. Supporting parents and protecting children are complementary goals, but when they conflict, the child's interests are paramount. (C) Educating the Public about ACEs and Related Science Lack of public awareness about ACEs perpetuates cycles of adversity. When individuals and communities remain unaware of how early trauma affects brain development, attachment, and foundational skills such as self-regulation, the root causes of difficulties remain unaddressed and intergenerational patterns continue unchallenged. In Scotland, where 71% of adults report at least one ACE (Scottish Health Survey, 2019), this knowledge gap contributes to societal costs that have been estimated to exceed £6 billion annually. Evidence from the Self-Healing Communities Model (SHCM) in Washington State demonstrates that educating residents about Neuroscience, Epigenetics, ACEs, and Resilience (NEAR science) can foster community empowerment and collective action for prevention (Porter et al., 2016). Several submissions to the Commission—including those from Social Current, the Royal College of GPs in Scotland, Scottish Attachment in Action, the Institute of Health Visiting, and Professor Christina Bethell—endorsed this 13 principle. As Social Current stated: "Improve awareness and education of brain science, ACEs and healthy child development for parents, professionals and the general public." The Commission recommends that Scotland develop a national public education programme on ACEs and NEAR science, delivered through accessible formats including community workshops, online resources, schools, and health services, to build public understanding and collective responsibility for child wellbeing. (D) Strengthening Professional Recognition of ACEs Inadequate professional recognition of ACEs perpetuates suffering. Survivors have consistently reported the experience that practitioners across both health and social care failed to explore the trauma roots behind presenting symptoms such as addiction, mental health difficulties, or involvement in crime. GPs and hospital doctors treated the symptoms—prescribing medication for anxiety, depression, or chronic pain—without ever inquiring about childhood experiences. Lived experience submissions to the Commission revealed repeated contacts with services without any inquiry into childhood adversity, leaving individuals feeling misunderstood and unsupported. Jay Haston, a survivor of child sexual abuse whose father was murdered when he was two and a half, described how signs of distress—including self-harm and fire-setting— went unrecognised despite contact with multiple services, contributing to a trajectory into crime and addiction (Haston, 2023). A Commissioner's interviews with 40 homeless individuals echoed this finding: all expressed a longing to have had "someone who believed in me," yet statutory interactions had never fostered that trust (Walsh, 2018). These accounts illustrate a systemic failure to connect presenting difficulties with their developmental origins. The Commission recommends that Scotland mandate ACE-informed training for all professionals working with children and families, emphasising NEAR science, trauma-informed inquiry, and reflective supervision—with training co-developed alongside those with lived experience of ACEs and evaluated through service user feedback. (E) Adopting a Whole-System Public Health Approach Fragmented systems exacerbate ACEs by failing to integrate prevention across sectors. When services operate in silos, early risks such as parental mental health difficulties or substance misuse are addressed—if at all—in isolation, without recognising their cumulative impact on children. Without holistic coordination, interventions remain reactive, missing opportunities to build resilience and prevent harm before it occurs.14 The Self-Healing Communities Model demonstrates that cross-sector collaboration, community leadership, and shared commitment to upstream prevention can achieve population-level change (Porter et al., 2016). In Scotland, the infrastructure is emerging: family hubs, the Promise, Getting It Right For Every Child (GIRFEC), and the new Public Sector Reform Strategy all emphasise integrated, preventive approaches. The challenge is to align these initiatives around a shared framework for ACE prevention, with clear accountability and sustained investment. The Commission recommends that Scotland adopt a whole-system public health approach to ACE prevention, with cross-sector collaboration coordinated through family hubs, shared data systems, and a national framework that embeds prevention as a core objective across health, education, social work, justice, housing, and employment services. This approach would support the Commission's goal of reducing ACEs by at least 70% for the next and all future generations—a transformation that is both achievable and essential for Scotland's future. References • Abramovaite, J., Bandyopadhyay, S., & Dixon, L. (2015). The dynamics of intergenerational family abuse: A focus on child maltreatment and violence and abuse in intimate relationships. Journal of Interdisciplinary Economics, 27(2), 160–174. • Afifi, T. O., Mota, N., Sareen, J., & MacMillan, H. L. (2017). The relationships between harsh physical punishment and child maltreatment in childhood and intimate partner violence in adulthood. BMC Public Health, 17(1), 493. • Arnsten, A. F. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience, 10(6), 410–422. • Asghari, M., Connolly, J., & Cochrane-Brink, K. (2021). Peer and dating aggression among early adolescent boys and girls admitted to a secure inpatient psychiatric unit: Links with maltreatment. Journal of Aggression, Maltreatment & Trauma, 30(2), 154–174. • Baldry, A. C. (2007). It does affect me: Disruptive behaviours in preadolescents directly and indirectly abused at home. Journal of European Psychology. • Bellis, M. A., Hughes, K., Cresswell, K., & Ford, K. (2023). Comparing relationships between single types of adverse childhood experiences and health-related outcomes: A combined primary data study of eight cross sectional surveys in England and Wales. BMJ Open, 13(4), e072916.15 • Bhushan, D., Kotz, K., McCall, J., Wirtz, S., Gilgoff, R., Dube, S. R., Powers, C., Olson-Morgan, J., Galeste, M., Patterson, K., Harris, L., Mills, A., Bethell, C., & Burke Harris, N. (2020). Roadmap for Resilience: The California Surgeon General's Report on Adverse Childhood Experiences, Toxic Stress, and Health. Office of the California Surgeon General. https://doi.org/10.48019/PEAM8812 • Biederman, J., Petty, C. R., Clarke, A., Lomedico, A., & Faraone, S. V. (2011). Predictors of persistent ADHD: An 11-year follow-up study. Journal of Psychiatric Research, 45(2), 150–155. • Brown, N. M., Brown, S. N., Briggs, R. D., Germán, M., Belamarich, P. F., & Oyeku, S. O. (2017). Associations between adverse childhood experiences and ADHD diagnosis and severity. Academic Pediatrics, 17(4), 349–355. • Buchanan, A. (1996). Cycles of Child Maltreatment: Facts, Fallacies, and Interventions. Wiley. • Burke, N. J., Hellman, J. L., Scott, B. G., Weems, C. F., & Carrion, V. G. (2011). The impact of adverse childhood experiences on an urban pediatric population. Child Abuse & Neglect, 35(6), 408–413. https://doi.org/10.1016/j.chiabu.2011.02.006 • Calem, M., Bromis, K., McGuire, P., Morgan, C., & Kempton, M. J. (2017). Meta analysis of associations between childhood adversity and hippocampus and amygdala volume in non-clinical and general population samples. NeuroImage: Clinical, 14, 471–479. • Carpenter, G. L., & Stacks, A. M. (2009). Developmental effects of exposure to intimate partner violence in early childhood: A review of the literature. Children and Youth Services Review, 31(8), 831–839. • Chapman, D. P., Whitfield, C. L., Felitti, V. J., Dube, S. R., Edwards, V. J., & Anda, R. F. (2004). Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82(2), 217–225. • Cprek, S. E., Williamson, L. H., McDaniel, H., Brase, R., & Williams, C. M. (2020). Adverse childhood experiences (ACEs) and risk of childhood delays in children ages 1–5. Child and Adolescent Social Work Journal, 37(1), 15–24. • D'Antoine, M., Malvaso, C., Delfabbro, P., & O'Connor, J. (2022). Suicidal behaviour in Aboriginal and non-Aboriginal young men under custodial youth justice supervision: Understanding the role of adverse childhood experiences. Psychiatry, Psychology and Law, 29(6), 953–975.16 • Dean, B. B., Calimlim, B. M., Kindermann, S. L., Khandker, R. K., & Tinkelman, D. (2009). The impact of uncontrolled asthma on absenteeism and health-related quality of life. Journal of Asthma, 46(9), 861–866. • De Venter, M., Demyttenaere, K., & Bruffaerts, R. (2013). The relationship between adverse childhood experiences and mental health in adulthood: A systematic literature review. Tijdschrift voor Psychiatrie, 55(4), 259–268. • DiGangi, M. J., & Negriff, S. (2020). The implementation of screening for adverse childhood experiences in pediatric primary care. Journal of Pediatrics, 222, 174– 179.e2. • Dodaj, A. (2020). Children witnessing domestic violence. Journal of Children's Services, 15(3), 161–174. • Dube, S. R., Felitti, V. J., Dong, M., Chapman, D. P., Giles, W. H., & Anda, R. F. (2003). Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The Adverse Childhood Experiences Study. Pediatrics, 111(3), 564–572. https://doi.org/10.1542/peds.111.3.564 • English, D. J., Marshall, D. B., & Stewart, A. J. (2003). Effects of family violence on child behavior and health during early childhood. Journal of Family Violence, 18(1), 43–57. • Farrington, D. P. (1991). Childhood aggression and adult violence: Early precursors and later-life outcomes. In D. J. Pepler & K. H. Rubin (Eds.), The Development and Treatment of Childhood Aggression (pp. 5–29). Lawrence Erlbaum Associates. • Felitti, V. J., & Anda, R. F. (2010). The relationship of adverse childhood experiences to adult medical disease, psychiatric disorders, and sexual behavior: Implications for healthcare. In R. Lanius, E. Vermetten, & C. Pain (Eds.), The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic (pp. 77–87). Cambridge University Press. • Fitton, L., Yu, R., & Fazel, S. (2018). Childhood maltreatment and violent outcomes: A systematic review and meta-analysis of prospective studies. Trauma, Violence, & Abuse, 21(4), 754–768. • Flaherty, E. G., Thompson, R., Dubowitz, H., Harvey, E. M., English, D. J., Black, M. M., Proctor, L. J., & Everson, M. D. (2013). Adverse childhood experiences and child health in early adolescence. JAMA Pediatrics, 167(7), 622–629. • Freisthler, B., Wolf, J. P., Wiegmann, W., & Kepple, N. J. (2021). Drug use behaviors and the relation to child maltreatment perpetration among a high-risk 17 sample of mothers. Journal of Interpersonal Violence, 36(5–6), NP1978–NP2000. https://doi.org/10.1177/0886260518757012 • Gardner, M. J., Thomas, H. J., & Erskine, H. E. (2019). The association between five forms of child maltreatment and depressive and anxiety disorders: A systematic review and meta-analysis. Child Abuse & Neglect, 96, 104082. • Goff, B., Gee, D. G., Telzer, E. H., Humphreys, K. L., Gabard-Durnam, L., Flannery, J., & Tottenham, N. (2013). Reduced nucleus accumbens reactivity and adolescent depression following early-life stress. Neuroscience, 249, 129–138. • Gong, J., Zhou, L., Zhao, L., Zhang, S., Chen, Z., & Liu, J. (2022). Epidemiology of childhood witnessing domestic violence and exploration of its relationships with affective lability and suicide attempts in Chinese young adults. Journal of Interpersonal Violence, 37(23–24), NP22834–NP22863. • González, R. A., Kallis, C., Ullrich, S., Barnicot, K., Keers, R., & Coid, J. W. (2016). Childhood maltreatment and violence: Mediation through psychiatric morbidity. Child Abuse & Neglect, 52, 70–84. • Gregory, A., Arai, L., MacMillan, H. L., Howarth, E., & Shaw, A. (2020). Children's experiences and needs in situations of domestic violence: A secondary analysis of qualitative data from adult friends and family members of female survivors. Health & Social Care in the Community, 28(2), 602–614. • Haston, J. (2023). Written submission to the Scottish Commission of Inquiry on Delivery of 70/30. • Herrenkohl, T. I., Fedina, L., Roberto, K. A., Raquet, K. L., Hu, R. X., Rousson, A. N., & Mason, W. A. (2022). Child maltreatment, youth violence, intimate partner violence, and elder mistreatment: A review and theoretical analysis of research on violence across the life course. Trauma, Violence, & Abuse, 23(1), 314–328. • Hogg, B., Gardoki-Souto, I., Valiente-Gómez, A., Ribeiro Rosa, A., Fortea, L., Radua, J., Amann, B. L., & Moreno-Alcázar, A. (2023). Psychological trauma as a transdiagnostic risk factor for mental disorder: An umbrella meta-analysis. European Archives of Psychiatry and Clinical Neuroscience, 273(2), 397–410. https://doi.org/10.1007/s00406-022-01495-5 • Hosking, G., & Walsh, I. (2005). Violence and What to Do About It (WAVE Report). WAVE Trust. • Hosking, G., & Walsh, I. (2013). Conception to Age 2: The Age of Opportunity. WAVE Trust/Department for Education. https://www.wavetrust.org/Handlers/Download.ashx?IDMF=f2c91a81-56a5- 47e8-9b79-48fd3b48276218 • Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., ... & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), e356–e366. • Hughes, K., Ford, K., Bellis, M. A., Glendinning, F., Harrison, E., & Passmore, J. (2021). Health and financial costs of adverse childhood experiences in 28 European countries: A systematic review and meta-analysis. The Lancet Public Health, 6(11), e848–e857. • Huth-Bocks, A. C., Levendosky, A. A., Theran, S. A., & Bogat, G. A. (2004). The impact of domestic violence on mothers' prenatal representations of their infants. Infant Mental Health Journal, 25(2), 79–98. • Insana, S. P., Banihashemi, L., Herringa, R. J., Kolko, D. J., & Germain, A. (2016). Childhood maltreatment is associated with altered frontolimbic neurobiological activity during wakefulness in adulthood. Development and Psychopathology, 28(2), 551–564. • Jimenez, M. E., Wade, R., Lin, Y., Morrow, L. M., & Reichman, N. E. (2016). Adverse experiences in early childhood and kindergarten outcomes. Pediatrics, 137(2), e20151839. • Jimenez, M. E., Wade, R., Schwartz-Soicher, O., Lin, Y., & Reichman, N. E. (2017). Adverse childhood experiences and ADHD diagnosis at age 9 years in a national urban sample. Academic Pediatrics, 17(4), 356–361. • Kertesz, M., Fogden, L., & Humphreys, C. (2021). Domestic violence and the impact on children. In The Routledge International Handbook of Domestic Violence and Abuse (pp. 128–140). Routledge. • Khemthong, O., & Chutiphongdech, T. (2021). Domestic violence and its impacts on children: A concise review of past literature. Asia Social Issues, 14(6), 249759–12. • Kolar, D. R., Monteleone, A. M., Cascino, G., Ertl, S., Meule, A., Naab, S., & Voderholzer, U. (2024). Pathways between child maltreatment, psychological symptoms, and life satisfaction: A network analysis in adolescent inpatients. Research on Child and Adolescent Psychopathology, 52(6), 969–982. • Lackova Rebicova, M., Dankulincova Veselska, Z., Husarova, D., Madarasova Geckova, A., van Dijk, J. P., & Reijneveld, S. A. (2019). The number of adverse childhood experiences is associated with emotional and behavioral problems among adolescents. International Journal of Environmental Research and Public Health, 16(13), 2446.19 • Leza, L., Siria, S., López-Goñi, J. J., & Fernandez-Montalvo, J. (2021). Adverse childhood experiences (ACEs) and substance use disorder (SUD): A scoping review. Drug and Alcohol Dependence, 221, 108563. • Lloyd, M. (2018). Domestic violence and education: Examining the impact of domestic violence on young children, children, and young people and the potential role of schools. Frontiers in Psychology, 9, 2094. • Mackes, N. K., Golm, D., Sarkar, S., Kumsta, R., Rutter, M., Fairchild, G., ... & ERA Young Adult Follow-up Team. (2020). Early childhood deprivation is associated with alterations in adult brain structure despite subsequent environmental enrichment. Proceedings of the National Academy of Sciences, 117(1), 641–649. • McCaffrey, A. (2023). Oral presentation to Scottish Commission of Inquiry on Delivery of 70/30. • McGuigan, W. M., Luchette, J. A., & Atterholt, R. (2018). Physical neglect in childhood as a predictor of violent behavior in adolescent males. Child Abuse & Neglect, 79, 395–400. • Mittal, K. (2020). Impact of domestic violence on children. International Journal of Innovative Science and Research Technology, 5(5). • Nelson, C. A., & Gabard-Durnam, L. J. (2020). Early adversity and critical periods: Neurodevelopmental consequences of violating the expectable environment. Trends in Neurosciences, 43(3), 133–143. • Ofsted. (2011). Ages of Concern: Learning Lessons from Serious Case Reviews. https://www.gov.uk/government/publications/ages-of-concern-learning lessons-from-serious-case-reviews • Oliveira, N. C. D. S., Bastos, A. F., Serpeloni, F., & de Assis, S. G. (2025). Transgenerational effects of violence in adolescents exposed to grandmaternal intimate partner violence during pregnancy: Heart rate variability and DNA methylation. Behavioural Brain Research, 497, Article 115886. https://doi.org/10.1016/j.bbr.2025.115886 • Øverlien, C. (2010). Children exposed to domestic violence: Conclusions from the literature and challenges ahead. Journal of Social Work, 10(1), 80–97. • Park, Y. M., Shekhtman, T., & Kelsoe, J. R. (2020). Effect of the type and number of adverse childhood experiences and the timing of adverse experiences on clinical outcomes in individuals with bipolar disorder. Brain Sciences, 10(5), 254.20 • Pingley, T. (2017). The impact of witnessing domestic violence on children: A systematic review. • Plant, D. T., Pariante, C. M., Sharp, D., & Pawlby, S. (2017). Association between maternal childhood trauma and offspring childhood psychopathology: Mediation analysis from the ALSPAC cohort. British Journal of Psychiatry, 211(3), 144–150. https://doi.org/10.1192/bjp.bp.117.198556 • Porter, L., Martin, K., & Anda, R. (2016). Self-Healing Communities: A Transformational Process Model for Improving Intergenerational Health. Robert Wood Johnson Foundation. https://www.rwjf.org/en/insights/our research/2016/06/self-healing-communities.html • Purwanti, A., & Tridewiyanti, K. (2019). Stop child marriage and eliminate sexual violence against women & children. Thafa Media. • Robles, A., Gjelsvik, A., Hirway, P., Vivier, P. M., & High, P. (2019). Adverse childhood experiences and protective factors with school engagement. Pediatrics, 144(2), e20182945. • Santoso, A. B. (2019). Domestic violence (DV) against women: A social work perspective. Komunitas, 10(1), 39–57. • Scheeringa, M. S., & Zeanah, C. H. (1995). Symptom expression and trauma variables in children under 48 months of age. Infant Mental Health Journal, 16(4), 259–270. • Schilling, E. A., Aseltine Jr, R. H., & Gore, S. (2007). Adverse childhood experiences and mental health in young adults: A longitudinal survey. BMC Public Health, 7(1), 30. • Schore, A. N. (2016). Affect Regulation and the Origin of the Self: The Neurobiology of Emotional Development. Routledge. • Scottish Government. (2019). The Scottish Health Survey 2019. https://www.gov.scot/publications/scottish-health-survey-2019-volume-1- main-report/ • Scottish Government. (2025). Scotland's Population Health Framework 2025– 2035. https://www.gov.scot/publications/scotlands-population-health framework/ • Scottish Government. (2025). Scotland's Public Service Reform Strategy: Delivering for Scotland. https://www.gov.scot/publications/scotlands-public service-reform-strategy-delivering-scotland/21 • Setiawan, N. H., Devi, S. S., Damayanti, L., Pramudya, F., & Antoni, H. (2023). The impact of domestic violence on victims: A comprehensive analysis. Civilia: Journal of Legal and Citizenship Education Studies, 12(1), 45–58. • Stempel, H., Cox-Martin, M., Bronsert, M., Dickinson, L. M., & Allison, M. A. (2017). Chronic school absenteeism and the role of adverse childhood experiences. Academic Pediatrics, 17(8), 837–843. • Streeck-Fischer, A., & van der Kolk, B. A. (2000). Down will come baby, cradle and all: Diagnostic and therapeutic implications of chronic trauma on child development. Australian & New Zealand Journal of Psychiatry, 34(6), 903–918. • Taillieu, T. L., Brownridge, D. A., Sareen, J., & Afifi, T. O. (2016). Childhood emotional maltreatment and mental disorders: Results from a nationally representative adult sample from the United States. Child Abuse & Neglect, 59, 1–12. • Teicher, M. H., & Samson, J. A. (2013). Childhood maltreatment and psychopathology: A case for ecophenotypic variants as clinically and neurobiologically distinct subtypes. American Journal of Psychiatry, 170(10), 1114–1133. • Teicher, M. H., Anderson, C. M., & Polcari, A. (2012). Childhood maltreatment is associated with reduced volume in the hippocampal subfields CA3, dentate gyrus, and subiculum. Proceedings of the National Academy of Sciences, 109(9), E563–E572. • Thakur, N., Hessler, D., Koita, K., Ye, M., Benson, M., Gilgoff, R., Bucci, M., Long, D., & Burke Harris, N. (2020). Pediatrics adverse childhood experiences and related life events screener (PEARLS) and health in a safety-net practice. Child Abuse & Neglect, 108, 104685. • Turner, S., Taillieu, T., Cheung, K., & Afifi, T. O. (2017). The relationship between childhood sexual abuse and mental health outcomes among males: Results from a nationally representative United States sample. Child Abuse & Neglect, 66, 64–72. • Turney, K. (2020). Cumulative adverse childhood experiences and children's health. Children and Youth Services Review, 119, 105538. • UNICEF. (2024). Over 370 million girls and women globally subjected to rape or sexual assault as children. https://www.unicef.org/press-releases/over-370- million-girls-and-women-globally-subjected-rape-or-sexual-assault-children • U.S. Department of Health and Human Services. (2020). Adverse Childhood Experiences: NSCH Data Brief. Health Resources and Services Administration, 22 Maternal and Child Health Bureau. https://mchb.hrsa.gov/sites/default/files/mchb/data-research/nsch-ace databrief.pdf • Van der Put, C. E., & De Ruiter, C. (2016). Child maltreatment victimization by type in relation to criminal recidivism in juvenile offenders. BMC Psychiatry, 16(1), 24. • Vyas, A., Mitra, R., Shankaranarayana Rao, B. S., & Chattarji, S. (2002). Chronic stress induces contrasting patterns of dendritic remodeling in hippocampal and amygdaloid neurons. Journal of Neuroscience, 22(15), 6810–6818. • Walsh, I. (2018). Age 2 to 18: Systems to Protect Children from Severe Disadvantage. WAVE Trust. • Weaver, I. C., Cervoni, N., Champagne, F. A., D'Alessio, A. C., Sharma, S., Seckl, J. R., Dymov, S., Szyf, M., & Meaney, M. J. (2004). Epigenetic programming by maternal behavior. Nature Neuroscience, 7(8), 847–854. • Weaver, I. C. G., Meaney, M. J., & Szyf, M. (2006). Maternal care effects on the hippocampal transcriptome and anxiety-mediated behaviors in the offspring that are reversible in adulthood. Proceedings of the National Academy of Sciences, 103(9), 3480–3485. • Widom, C. S. (1989). The cycle of violence. Science, 244(4901), 160–166. • Wilson, P., Bradshaw, P., Tipping, S., Henderson, M., Der, G., & Minnis, H. (2013). What predicts persistent early conduct problems? Evidence from the Growing Up in Scotland cohort. Journal of Epidemiology & Community Health, 67(1), 76–80. https://doi.org/10.1136/jech-2011-200765 • World Health Organization Europe. (2013). European Report on Preventing Child Maltreatment. WHO Regional Office for Europe.
Relational Health Risks (RHR) Social Health Risks (SHR) % with Mental, Emotional or Behavioural Problems
No RHR No SHR 15.1% No RHR 2–4 SHR 28.8% 2–4 RHR No SHR 42.3% 2–4 RHR 2–4 SHR 60.4%3 The average impact of the relational risks was almost double, at 29.4 percentage points (42.3−15.1 = 27.2%, 60.4−28.8 = 31.6%) those of social risks at 15.9 percentage points (28.8−15.1 = 13.7%, 60.4−42.3 = 18.1%). Again, the most favourable outcomes occur when parents are free from both social and relational risks. 14.4.3 Bellis et al. (2017) In a study of 7,047 UK adults, from four separate UK regions, Bellis and colleagues compared the impact of (1) Deprivation (by the five quintiles of deprivation), (2) a positive aspect of parenting — the presence or absence of an always available (supportive) adult, and (3) a negative aspect of family life, the number of adverse childhood experiences, or ACEs in the lives of the adults studied. The measures examined were three individual health-harming behaviours (daily smoking, poor diet and regular heavy drinking); the presence of two or more health harming behaviours; and mental wellbeing. Using associations as a proxy for impacts, the relative impacts of deprivation, supportive parenting and adverse family factors varied according to the behaviours measured. Relative to the family factors, deprivation had a low impact on four of the measures, but a high impact on daily smoking (though still less than half the impact of 4 or more ACEs). The presence of an Always Available Adult had a positive effect on all measures, but a particularly high impact on mental wellbeing (though still just above half of the impact of four or more ACEs). By far the most powerful factor of all was the presence of four or more ACEs, dwarfing the impact of deprivation. Consistently, on all five measures, being in the least deprived economic quintile but with four or more ACEs, produced worse life outcomes than being in the most deprived economic quintile, with zero ACEs. Conclusion. Good parenting and relational security matter significantly more to a child’s development than income alone; good parenting plus reduced poverty deliver the strongest mental, emotional, educational and health outcomes. These findings suggest that while poverty matters, the decisive variable is relational capacity — and that building relational capacity should be the primary focus, supported by measures that reduce material stress.4 14.4.4 Why Strong Relationships Buffer So Effectively The three studies above show that strong relationships buffer against poverty and inequality — but why do they buffer so effectively? The answer lies in how early relationships shape the stress response system. When children experience consistent, attuned caregiving — even in contexts of material hardship — they develop: • Regulated stress response systems that can handle adversity without becoming overwhelmed • Secure attachment providing an internal sense of safety and worth • Core capabilities (self-regulation, emotional control, executive function) that enable them to navigate challenges • Positive internal working models of relationships that support resilience Good parenting is inherently rewarding for both parent and child — it generates love, joy, and meaning that sustain families through hardship. Conversely, when parents lack these internal resources — often due to their own ACE histories — the additional stress of poverty and inequality overwhelms limited coping capacity, making responsive caregiving much harder to sustain. 14.5 Understanding the Mechanisms 14.5.1 Why GDP Growth Alone Hasn’t Solved Poverty Between 1950 and 2000, UK GDP per capita rose four-fold in real terms. Yet child abuse rates remained flat and violence tripled. Increased prosperity did not deliver protection. Other factors must have been at play, overwhelming the benefits of improved income levels. It is not axiomatic that reduced poverty equates with improved social outcomes. The anthropologist Levinson (1989) studied 80 societies around the world. Among these he found extremely poor societies (measured by material deprivation) with extremely low levels of violence or child abuse. What distinguished these societies were their cultural norms of respect, non-violence and gender equality. Their strong cultural norms around child-rearing and community support created the relational conditions for healthy development despite poverty. 14.5.2 Why Money Alone Is Not Enough The Baby’s First Years experiment (Magnuson et al., 2022), in four regions of the USA, gave 1,000 low-income mothers either $333 per month or $20 per month for four years. Despite a cumulative $15,000 difference for the $333 group, mothers randomised into the high-cash gift category did not show improvement in subjective well-being, 5 parenting stress, or health outcomes among their children, nor (beyond the first year) the quality of play with their infants. The lesson is not that money is irrelevant — families used it for essentials — but that income alone cannot transform developmental trajectories. 14.5.3 The Inequality Question — What the Evidence Shows What about inequality? Some researchers, notably Wilkinson and Pickett in The Spirit Level, argue that inequality itself causes poor outcomes through psychosocial stress and status anxiety. The UK evidence on this is equivocal. Income inequality in the UK fell between the 1950s and the 1970s; yet violent offences per 100,000 population in England & Wales rose from 47 in 1950 to 146 in 1970 (more than threefold), to 271 in 1980 (more than fivefold) — while inequality was reducing. Subsequently, by 2000, when inequality had risen again (the Gini coefficient rose sharply between 1979 and 1991), violence continued to rise, reaching 735 per 100,000 population (over 15-fold) by 2000. This pattern suggests that if inequality harms outcomes, it does not operate through a simple, direct mechanism. Just as greater prosperity did not improve these measures of social dysfunction, there is no evidence from these UK data that reducing inequality, of itself, reduces social dysfunction. 14.5.4 Control and Agency — A More Powerful Framework Bruce Perry’s synthesis of the Whitehall Studies and primate research offers a more nuanced framework for understanding how inequality might affect outcomes (Szalavitz & Perry, 2010). What matters most, the evidence suggests, is not hierarchy per se, but lack of control, unpredictability, and chronic threat. Marmot’s Whitehall Studies examined 18,000 British civil servants — importantly, none of whom were poor; all had secure employment and universal healthcare. Yet they found a massive health gradient: lowest-ranking civil servants were four times more likely to die at ages 40–64 than those at the top (Marmot et al., 1978, 1984, 1991). This gradient tracked rank precisely. Michael Marmot’s analysis found that the strongest predictor of ill-health was lack of control over work — including lack of variety, inability to use or develop skills, and accountability for outcomes over which one had little influence (Marmot, 2008). This pattern held even after controlling for smoking, diet, and other lifestyle factors. Robert Sapolsky’s baboon research (Sapolsky, 1990) provided experimental confirmation. Low-ranking baboons showed stress-related pathology — elevated stress hormones, high blood pressure, weakened immunity — despite abundant food and few predators. Critically, Sapolsky observed a natural experiment: after tuberculosis killed 6 the most aggressive males in one troop, the remaining males maintained their hierarchy but dramatically reduced bullying of subordinates. The stress-related pathology of low ranking males disappeared — even though they remained low-ranking. The hierarchy remained; the chronic stress did not. This framework helps explain the inequality data: Rising inequality may harm primarily when it translates into reduced control, increased precarity, and diminished agency — particularly for parents already carrying trauma or insecure attachment from their own childhoods. Inequality creates conditions where stressed parents feel increasingly powerless, which impairs exactly the emotional regulation and responsive caregiving that children need. 14.5.5 How Poverty and Inequality Interact with Relational Capacity The evidence converges on a crucial insight: poverty and inequality appear to harm children primarily when parents lack strong internal relational resources — usually because of their own ACE histories, unresolved trauma, or insecure attachment models. When parents have strong relational capacity (secure attachment history, positive parenting models, emotional regulation skills), then although poverty may still generate hardship and stress: • The parenting itself is intrinsically rewarding — generating love, connection, and meaning • Parents maintain responsive caregiving despite material constraints • Children develop secure attachment and core skills • This explains the Millennium Cohort finding: 58% good development with persistent poverty + positive parenting When parents have compromised relational capacity (ACE history, trauma, poor parenting models, insecure attachment): • Material stress and lack of control overwhelm limited coping reserves • Poverty and precarity trigger trauma responses • Parents struggle to maintain attuned caregiving • Children experience inconsistent care, potential ACEs, poor skill development • This explains the Millennium Cohort 19% outcome from persistent poverty + poor parenting The poverty is constant in both scenarios; parenting quality is the decisive variable. This is not about blaming parents — those with compromised capacity often carry 7 intergenerational trauma and deserve substantial support. Rather, it clarifies where intervention achieves maximum impact: building relational capacity is the primary lever, supported by structural measures that reduce stress and enable parents to access and benefit from relationship-based support. 14.6 Why Early Skills Matter — And How to Build Them If poverty and inequality harm primarily by impairing skill development through stressed parenting, then tackling poverty most effectively requires understanding how these skills form — and building them through strengthened relationships. Decades of longitudinal research converge on the same conclusion: early relationships and skill development are the decisive mechanisms linking childhood experience to adult outcomes. The analyses of the Nobel Prize winning economist James Heckman (Heckman, 2000, 2007, 2008, 2011) demonstrate that: • Early skill formation — especially non-cognitive skills such as self-control, perseverance, and emotional regulation — predicts later success more strongly than income. • These skills are built primarily through early relationships. • Returns on investment in early skill development average 7–10% annually, exceeding most financial investments. The Dunedin Study (Moffitt et al., 2011) showed that children with low self-control at age three accounted for the majority of negative outcomes in adulthood — unemployment, poor health, crime. They perform poorly in school (a precursor of adult poverty), accumulate less wealth, exhibit less skilled parenting tactics, and are more likely to have had children who faced similar challenges. This suggests that low self control in one generation can perpetuate difficulties and disadvantages to the next generation, reinforcing the importance of addressing self-control in early childhood as a means of breaking the cycle of poverty. Crucially, the associations remained significant even after accounting for the participants’ social class and intelligence. The researchers summarised their findings thus: Our 40-year study of 1,000 children revealed that childhood self-control strongly predicts adult success, in people of high or low intelligence, in rich or poor. Carneiro (2007) at the LSE found that non-cognitive skills at age 11 predicted education, employment status, earnings, health, and family stability into middle age. This impact did not differ in any systematic way across particular subgroups including parental education, or father’s socioeconomic status.8 The Mannheim Study of Children at Risk (MARS) (Blomeyer et al., 2008) found that individual differences between children in cognitive and noncognitive capabilities are detectable at 3 months of age, then amplify between 3 months and 11 years. They are consistently associated with socio-emotional (not socio-economic) home resources, and that noncognitive abilities promote cognitive abilities. The Oxbridge report by Helmers & Patnam (2011), on the formation and evolution of childhood skill acquisition, found that parental investment significantly improves cognitive and non-cognitive skill levels at all ages. Crucially, they identified a pathway from parental care during pregnancy and onwards, to child health at age 1, to cognitive ability at age 5, reinforcing the need for early medical and parental support. In terms of what matters in ‘parental investment’ the authors quote Waldfogel (2006): ‘maternal sensitivity is the most important predictor of child social and emotional development’. This is exactly the same conclusion as reached in our current study. Cunha and colleagues (2005) summarised the process thus: “Skill formation is a life cycle process. It starts in the womb and goes on throughout life. Families play a role in this process that is far more important than the role of schools. Abilities are both inherited and created. Skill attainment at one stage of the life cycle raises skill attainment at later stages of the life cycle. Early investment facilitates the productivity of later investment. Early investments are not productive if they are not followed up by later investments. The returns to investing early in the life cycle are high. Remediation of inadequate early investments is difficult and very costly.” Thus, income supports opportunity, but relational capacity builds capability. This suggests that addressing poverty most effectively means building these early capabilities, not least parental sensitivity, through support for strengthened parent child relationships. 14.7 Breaking the Cycle of Poverty: Structural and Relational Solutions Together The evidence presented in sections 14.4 to 14.6 above converges on a clear conclusion that has profound implications for Scotland’s approach to tackling poverty and inequality. What the evidence tells us: • The Millennium Cohort, Bethell, and Bellis studies each suggest that relational factors have roughly twice the impact of material factors on child outcomes • The Baby’s First Years trial shows that cash transfers alone, without relational support, do not transform developmental trajectories9 • The Whitehall Studies and baboon research show that what harms is not hierarchy itself, but lack of control, unpredictability, and chronic threat • The interaction model (14.5.5) demonstrates that poverty and inequality harm primarily when they overwhelm parents who lack strong relational resources • Both the skill development research (14.6), and evidence from individuals with lived experience of poverty, show that the capabilities which enable people to escape poverty — self-regulation, executive function, emotional control, sense of agency — are built through the quality of early relationships, not purchased with money. The inescapable conclusion: Poverty and inequality cause great harm, but they harm most when they coincide with fragile relationships and compromised parenting capacity. Conversely, strong relational capacity buffers substantially against material hardship — enabling children to thrive despite poverty. What this means in practice: ‘Structural supports’ are measures that reduce material stress and increase control over one’s life — housing, transport, employment quality, food security, childcare access. ‘Relationship-centred interventions’ are programmes that build parenting capacity, strengthen parent-child bonds, and develop children’s core capabilities through early relationships. This means Scotland would benefit from pursuing a two-pronged strategy: relieve immediate material strain and build the early relational capacities that make future prosperity possible. Neither alone is sufficient; both together are essential. But — and this is crucial — the evidence is unequivocal that building relational capacity is the more powerful lever for transforming outcomes. This is not an argument against financial support; it is an argument for strategic prioritisation based on what the evidence shows actually works. Scotland’s limited resources should be allocated where they achieve maximum impact — and that means prioritising relationship-centred interventions alongside sustained action on child poverty targets, while maintaining structural supports that reduce stress and enable families to access and benefit from relational support. 14.7.1 Structural Supports — The Necessary Foundation Reducing material stress and increasing control are essential conditions for good parenting and healthy development. The most effective structural supports include: Housing: Safe, stable, affordable homes improve health, reduce stress, and enable nurturing routines. Transport: Access to reliable transport lowers ACE exposure by connecting families to work, services, and social support (Blair et al., 2019).10 Food and Nutrition: Adequate diet during pregnancy and early years supports brain development; free school meals and breastfeeding support are proven protectors. Employment Quality: The Whitehall Studies show that control over work — autonomy, skill use, meaningful decision-making — matters as much as pay for health outcomes. Addressing in-work poverty therefore requires living wage and secure contracts; genuine flexibility that gives workers control over schedules, where possible, not just employer flexibility; opportunities for skill development and progression that build agency; and respectful management practices that give workers voice in decisions affecting them. These measures directly address the control deficit that appears to mediate inequality’s harms. Childcare: High-quality, affordable childcare promotes early learning and enables parental employment. Reduced Bureaucratic Burden: Simplifying benefit systems and providing single access points restores dignity and saves families’ limited energy. These structural supports are essential — but they are enabling, not transformational, without the second component. 14.7.2 Relationship-Centred Interventions — The Highest-Impact Lever Evidence from decades of trials shows that interventions focused on parenting capacity and early relationships yield the largest and most enduring returns. The Perry Preschool and Abecedarian projects demonstrated that intensive early education combined with parent support increased education, earnings, and health while reducing crime, with returns on investment of 7:1 or higher. Family Nurse Partnership has shown significant positive effects in trials with high implementation fidelity, such as the VoorZorg trial in the Netherlands. Evidence from UK implementation has been more mixed, with some researchers questioning whether the model translates effectively to the UK context. Self-Healing Communities, a community-wide approach to preventing ACEs, shows cost-benefit ratios around 35:1. Together, these findings show that while structural measures remove obstacles, relationship-based programmes build the human foundations of prosperity. 14.7.3 The Investment Case The cost of ACEs to Scotland is estimated at £6 billion annually. Each £1 invested in prevention yields £7–10 in reduced reactive spending across health, education, justice, and social care. Redirecting a small proportion of existing budgets from late-stage crisis services to early prevention can fund this transformation at no additional net cost.11 The Perry Preschool Project demonstrates the return on investment precisely: high quality early intervention combining parenting support with developmental education produced benefits worth 7–10 times the cost when participants were followed to age 40. The Carolina Abecedarian Project showed similar returns tracked to age 35. 14.8 Case Study: Sweden — Integration at Scale Sweden demonstrates that the integration of structural and relational supports can work at national scale, achieving substantially better outcomes not by eliminating inequality entirely, but by ensuring structural supports actively enable relationship building. Family Centres: The Core Model At the heart of Sweden’s approach are Family Centres — a state-run initiative since the 1970s that integrates supports in one accessible location. Relational supports include parenting skills groups and individual guidance, parent groups starting when children are 1–2 months old, and maternity and child healthcare through which 99% of pregnant women access services, averaging 20 contacts with nurses; 98% of maternity clinics offer parenting education to first-time parents. Alongside these, structural supports are delivered in the same setting: training for unemployed parents, accessible childcare, integrated health, social and employment services, and extended paid parental leave that enables parents to focus on bonding with their infants. This is precisely the integration Scotland can pursue through Family Hubs: structural and relational supports together, universally accessible, non-stigmatising. Employment Quality: Building Control and Agency Sweden’s employment approach directly addresses the control and agency deficits that Marmot’s Whitehall Studies identify as key mechanisms linking inequality to poor health. Only 6.9% of employed Swedes live below the poverty line, compared with 18% in the UK. Seventy percent of the workforce is unionised (compared with 23% in the UK), protecting pay and conditions. Zero-hours contracts and gig economy exploitation are limited. Swedish workers experience greater predictability, autonomy, and sense that effort leads to reward — the psychological foundations needed for effective parenting. The Outcomes Sweden has not eliminated health inequality — life expectancy gaps between the most and least educated remain (2.9 years for women, 4.1 years for men). But these gaps are smaller than the UK’s (4.0 and 4.4 years respectively), and overall outcomes are dramatically better: • Infant mortality: 2.5 per 1,000 live births (UK: 5.1; Scotland: 3.6) • Teenage births: 1.6% (UK: 7.1%)12 • Adult obesity: 11% (UK: 23%) • Child mortality under age 4: half England’s rate What Scotland Can Learn Sweden proves the integration approach works at scale. The key insight is that structural and relational supports are integrated — not delivered separately — so that parents accessing healthcare receive parenting support, employment policies consider family needs, and services are universal but with progressive intensity for those who need more. Scotland can pursue Family Hubs modelled on Sweden’s Family Centres: delivering both structural navigation support and relationship-building in universally accessible, community-based settings, underpinned by recognition that building relational capacity is the primary lever for breaking intergenerational disadvantage. 14.9 Addressing Common Questions Some will worry that this approach downplays poverty. It does not. It treats poverty more seriously — by addressing how it damages children and by investing in what actually breaks the cycle. Others may fear it blames parents. On the contrary, it recognises that parenting under economic strain is extraordinarily hard, especially for those who experienced trauma themselves. These parents deserve more support, not less. Still others will argue that structural inequality must be solved first. But waiting to eliminate inequality before building relational capacity risks losing another generation. The evidence shows both must proceed together — and that building early skills delivers the greater long-term effect. 14.10 Conclusion: Aligning Compassion with Evidence Poverty and inequality remain among Scotland’s greatest moral challenges. But the evidence now offers a hopeful path. We can build a fairer, more prosperous Scotland — not only by redistributing resources, but by cultivating the human capabilities that allow families and communities to flourish. The data are unequivocal: • Poverty and inequality correlate with poor outcomes, but primarily through their impact on relationships and early skill formation. • Strong relationships and parental attunement buffer against those harms.13 • Relationship-centred prevention yields higher and longer-lasting returns than financial support alone. By aligning our substantial commitment to reducing poverty and inequality with clear evidence about how they harm children — and therefore how to address them most effectively — Scotland can achieve something remarkable: not just reduced child poverty statistics, but transformed life chances for every child. This is the promise of an evidence-led approach: better outcomes, achieved more efficiently, respecting both the dignity of families and the reality of constrained resources. It is how we truly honour the commitment that we are all Jock Tamson’s bairns — not through sentiment alone, but through ensuring every child has the early relationships and developed capabilities they need to thrive. The 70/30 objective — and far more — is now achievable for future generations of Scottish children, with benefits in perpetuity for Scottish adults — if we have the courage to align our compassion with our evidence. References Bellis, M. A., Hardcastle, K., Ford, K., Hughes, K., Ashton, K., Quigg, Z., & Butler, N. (2017). Does continuous trusted adult support in childhood impart life-course resilience against adverse childhood experiences — a retrospective study on adult health-harming behaviours and mental well-being. BMC Psychiatry, 17(1), 110. https://doi.org/10.1186/s12888-017-1250-y Bethell, C. D., Garner, A. S., Gombojav, N., Blackwell, C., Heller, L., & Mendelson, T. (2022). Social and relational health risks and common mental health problems among US children: The mitigating role of family resilience and connection to promote positive socioemotional and school-related outcomes. Child and Adolescent Psychiatric Clinics, 31(1), 45–70. Blair, A., Marryat, L., & Frank, J. (2019). How community resources mitigate the association between household poverty and the incidence of adverse childhood experiences. International Journal of Public Health, 64(7), 1059–1068. https://doi.org/10.1007/s00038-019-01258-5 Blomeyer, D., Coneus, K., Laucht, M., & Pfeiffer, F. (2008). Self-productivity and complementarities in human development: Evidence from the Mannheim Study of Children at Risk (IZA Discussion Paper No. 3734). Available at SSRN: https://ssrn.com/abstract=127893514 Bywaters, P., Bunting, L., Davidson, G., Hanratty, J., Mason, W., McCartan, C., & Steils, N. (2016). The relationship between poverty, child abuse and neglect: An evidence review. Joseph Rowntree Foundation. Carneiro, P., Crawford, C., & Goodman, A. (2007). The impact of early cognitive and non cognitive skills on later outcomes. Centre for the Economics of Education, London School of Economics. Cunha, F., Heckman, J. J., Lochner, L., & Masterov, D. V. (2005). Interpreting the evidence on life cycle skill formation (NBER Working Paper No. 11331). https://doi.org/10.3386/w11331 Heckman, J. J. (2000). Policies to foster human capital. Research in Economics, 54(1), 3–56. Heckman, J. J. (2007). The economics, technology, and neuroscience of human capability formation. Proceedings of the National Academy of Sciences, 104(33), 13250–13255. Heckman, J. J. (2008). The economics and psychology of inequality and human development [Marshall Lecture]. European Economics Association, Milan. Heckman, J. J. (2011). The American family in Black and White: A post-racial strategy for improving skills to promote equality. Daedalus, 140(2), 70–89. Helmers, C., & Patnam, M. (2011). The formation and evolution of childhood skill acquisition: Evidence from India. Journal of Development Economics, 95(2), 252–266. Kiernan, K. E., & Mensah, F. K. (2011). Poverty, family resources and children’s early educational attainment: The mediating role of parenting. British Educational Research Journal, 37(2), 317–336. Levinson, D. (1989). Family violence in cross-cultural perspective. Sage. Magnuson, K., Yoo, P., Duncan, G., Yoshikawa, H., Trang, K., Gennetian, L. A., Noble, K., et al. (2022). Can a poverty reduction intervention reduce family stress among families with infants? An experimental analysis. Available at SSRN: https://papers.ssrn.com/abstract=4188131 Marmot, M. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. World Health Organization. Marmot, M. G., Rose, G., Shipley, M., & Hamilton, P. J. S. (1978). Employment grade and coronary heart disease in British civil servants. Journal of Epidemiology and Community Health, 32(4), 244–249.15 Marmot, M. G., Shipley, M. J., & Rose, G. (1984). Inequalities in death — specific explanations of a general pattern? The Lancet, 323(8384), 1003–1006. Marmot, M. G., Davey Smith, G., Stansfeld, S., Patel, C., North, F., Head, J., White, I., Brunner, E., & Feeney, A. (1991). Health inequalities among British civil servants: The Whitehall II study. The Lancet, 337(8754), 1387–1393. Moffitt, T. E., Arseneault, L., Belsky, D., Dickson, N., Hancox, R. J., Harrington, H., Houts, R., Poulton, R., Roberts, B. W., Ross, S., Sears, M. R., Thomson, W. M., & Caspi, A. (2011). A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences of the United States of America, 108(7), 2693–2698. Sapolsky, R. M. (1990). Adrenocortical function, social rank, and personality among wild baboons. Biological Psychiatry, 28(10), 862–878. Szalavitz, M., & Perry, B. D. (2010). Born for love: Why empathy is essential — and endangered. William Morrow. Waldfogel, J. (2006). What children need. Harvard University Press.
Qualifications 50–80% hold bachelor’s or master’s degrees ~30% have degrees; minimum SVQ Level 3
Pay £35,000–50,000 £22,000–32,000 Staff turnover 5–10% 15–25%
Child outcomes Low inequality in development Higher gaps in deprived areas
19.4.2 The Nutbrown Review Recommendations The 2012 Nutbrown Review in England set out recommendations that remain relevant for Scotland: • Minimum Level 3 qualifications for all practitioners • Mandatory literacy and numeracy standards • Stronger training content focused on child development and play pedagogy • Graduate-led expertise in every setting • Clear career pathways with ongoing professional development 19.4.3 Scotland’s Progress and Remaining Challenges Scotland has made progress, particularly through graduate-led provision in many settings and the Realising the Ambition framework. The Government has expanded fully funded high-quality early learning and childcare, providing 1,140 hours per year for eligible children aged two, three, and four. Upstart Scotland noted that guidance already exists in “the excellent document Realising the Ambition: Being Me, which covers the age-range up to Primary 1/2,” and that with funded early learning from age three (age two for vulnerable children), it would not be difficult or expensive to introduce a kindergarten stage. However, fundamental challenges remain around workforce recruitment, training quality, pay levels, and professional status. As evidence from Section 11 concluded: “Implementing play-based kindergarten without addressing workforce quality will fail. Children will not develop the four foundational capacities through time in buildings or exposure to resources—they develop them through relationships with emotionally intelligent, developmentally informed, professionally supported adults.” 19.4.4 Implications for Scotland The Commission heard that transforming the early years workforce requires: • Rigorous training focused on child development, attachment, play pedagogy, and the emotional intelligence to build relationships with vulnerable families • Training that includes extended supervised placements and ongoing mentoring • Raising professional status, pay, training quality, and career pathways to reflect the developmental importance and complexity of work with young children• Investing in workforce capability and stability, including specialist training in child development, play-based learning, and relational pedagogy, supported by clear progression routes and sustained professional development 19.5 Family Centres and Integrated Services 19.5.1 The Case for Full Service Children’s Centres Professor Ted Melhuish provided extensive evidence on the value of integrated service delivery: “In the Early Childhood area, our research has shown that provision of ‘Full Service Children’s Centres’, of which there are very few in the UK (examples are in Manchester, Birmingham and London), when implemented well, are extremely successful in producing better outcomes for children in disadvantaged areas.” These centres encompass health services (including midwives and health visitors), early childcare, early childhood education, social services, family support, and parental support under one roof. Melhuish described the benefits: “When staff in such Centres are interviewed they report the environment is much better, with significantly better collaboration, better communication, better referrals and greater mutual respect between the different professions working there. They prefer this way of working. Referrals to other services are much easier.” A particular advantage is continuity across developmental stages: “Currently Health Visitors pick up problems of families very early on, but then lose contact with the families. The benefit of the proposed ‘Full Service Children’s Centres’ approach is that it allows these issues to be shared with other services, who engage with families later in a child’s journey. Working in the same location assists this.” 19.5.2 Evidence on Outcomes Evidence gathered by Grok confirmed the effectiveness of this model. The National Evaluation of Sure Start (NESS), led by Melhuish, found that three-year-olds in well established centres demonstrated better social behaviour, independence, and home learning environments. By age five, children showed improved school readiness and reduced behavioural problems. Long-term follow-up to age seven showed sustained health and education gains (Melhuish et al., 2005, 2008, 2010). For low-socioeconomic-status families, centres reduced inequalities, including better maternal mental health and employment outcomes. Cost-benefit analysis suggests £1 invested yields £1.50–3 in savings from reduced crime and health costs. The critical success factor is implementation quality. Early Sure Start had mixed results due to variable quality, but “fully established” centres following 2006 guidelines showed stronger effects.19.5.3 Staff Turnover and Career Structures Professor Melhuish identified a significant implementation challenge: “Staff turnover in Children’s Centres is currently a real problem which can be resolved by proper training, pay and status.” He recommended that centres be “associated with primary schools, supported by increased staff training and status, with a career structure for staff working in these centres.” 19.5.4 Community-Based Alternatives Several witnesses emphasised the importance of accessible, non-stigmatising community spaces even where full-service centres are not feasible. Alan Sinclair called for “an expanded network of ELCC which should look after parents as well as children” and “Family Centres or Wellbeing Centres with a range of professionals including health visitors, play therapists.” Dr Robin Balbernie described “family centres as the bedrock of all early intervention, from universal to very specialist.” Professor Robert Sege offered practical examples of engagement approaches: “Parent Café” sessions at accessible venues where parents can ask questions about parenting; “fussy baby clinics” which engage parents who need support and can receive parent-infant interaction therapy; and baby massage classes delivered by social services where informal chat builds relationships when babies fall asleep. Jackie Tolland described her organisation’s approach: “We have family hubs, and parents post-Covid had nowhere to go. We invite them to come in, with no conditions attached. They were isolated, frustrated, they had no money. Come in and have tea and toast and a natter.” 19.5.5 Current Scottish Investment The Scottish Government is investing £500 million in Whole Family Support, with £50 million allocated to the Whole Family Wellbeing Funding this year, which aims to deliver transformational change to improve holistic whole family support. 19.6 Working with Families 19.6.1 Strengths-Based Approaches A consistent theme throughout the evidence was the importance of working with families rather than doing to them. Tam Baillie articulated the principle: “Change the culture in our approach to working with children, young people and families to positive working with, rather than doing to.” Tony McDaid reinforced this: “We need to build high quality relationships with families and with children. This is done through professionals being beside families, rather than intervening, and through ensuring we are listening to the child’s voice.”Dr Robin Balbernie emphasised that “interventions should be strength-based and build on protective factors within and around the parents, e.g. proficiency, resilience and self esteem.” Research evidence supports this approach: “Practice that builds on people’s strengths is demonstrably more effective than approaches that emphasise problems, risks and the expertise of professionals.” 19.6.2 Assessment Frameworks Supporting Engagement Tam Baillie highlighted recent developments in assessment frameworks that support constructive family engagement: “Graded Care tools have been developed by Action for Children and NSPCC. Evaluations of Graded Care show that it ‘contributes to a constructive working relationship between practitioners and families’. Signs of Safety is another assessment framework promoting positive engagement with families with an extensive body of evaluations over a long period.” He noted that in Scotland, both approaches have been adopted in many local authority areas, coinciding with reductions in the number of looked-after children from 16,231 in 2011 to 13,255—the lowest figure since 2006. 19.6.3 Engaging Hard-to-Reach Families Several witnesses addressed the challenge of engaging families who do not readily access services. Professor Daniel Shaw identified the need to “engage families—how do we make it easier for families to access services? For example, by using locations they already trust.” Mhairi Cavanagh noted that “parents not ready to reach out to services. The priority needs to be on building trusting relationship with professionals.” The RCGPS emphasised that “continuity of relationships is important, particularly as establishing trust is an issue for those who are parents and who have themselves had adverse childhood experiences.” Adam Burley offered a striking analogy for the barriers faced by those with relational injury: “Address barriers to psychological therapy which is founded on the expectation people can build trusting relationships. Equivalent to putting services for people in wheelchairs on the third floor with no lift. Be aware people with relational injury present in a way which doesn’t evoke care and sympathy.” 19.6.4 Engaging Fathers Mhairi Cavanagh highlighted a significant gap in current practice: “Dads are a key part of families but are often overlooked by services. The relationship between midwives and fathers, and health visitors and fathers is non-existent. There are strategies within FNP which are good at engaging fathers, e.g. specific materials for dads and an emphasis on building relationships with fathers. There is a need for policies to support father involvement, e.g. paternity policies.”19.6.5 Key Principles for Effective Family Work Professor Jane Barlow identified core principles for effective family intervention. Services should: • Address multiple domains of family functioning and deal with the wider family as well as the individual • Be delivered in the home using individualised goals • Set clear targets for change • Focus on the parent’s capacity for mentalisation and development of relationship with key workers Joy Barlow emphasised additional operational principles: understanding of connectedness between parents, children, and professionals; positive feedback to parents that is self affirming and strengths-based; continuity of care with programmes that should not be time-limited; willingness to stay with the difficult stuff; low caseloads; home-based outreach; and recognition that scrutiny and surveillance can be barriers to engagement and help. 19.6.6 One Family, One Plan Alan Sinclair articulated a fundamental service design principle: “The importance of 1 family, 1 plan rather than multiple service involvement and multiple plans which is confusing and overwhelming for families.” Professor Helen Minnis expanded on the challenge: “There is a service gap, but also difficulty navigating services.” She recommended “implementing a role of a professional to help families to navigate across services—often they don’t know what services are available.” This echoes Professor Ted Melhuish’s proposal for “Child Development workers, who work with families who need support, over extended periods of time—e.g. a health visitor who is retrained as a Child Development worker, who works with families from birth to age 16, so there is continuing support for the children from the same person over a period of years.” 19.7 Professional Training 19.7.1 The Scale of the Training Challenge Throughout the evidence gathered by the Commission, training emerged as a critical enabler—or barrier—to effective prevention. With 41 written submissions addressing professional training, the evidence demonstrates that transformation requires systematic workforce development across all professionals working with families, not just specialist early years workers. Professor Christina Bethell captured the scope: “Universal training on trauma informed and healing centred care for all government, community-based organisation, healthcare, education, child welfare, and family-serving systems staff.” Jay Haston reinforced this from a lived-experience perspective, calling for “mandatory trauma-informed practice training for all adults who come into contact with children (e.g. lunchtime staff, school cleaners etc.). This would ensure there are available and responsive adults working with children, facilitating identification of issues and disclosures.” 19.7.2 Core Training Content The evidence identified several essential elements for professional training: Attachment and child development: Nurture International called to “increase understanding of child development across professionals working with children and families. This should include attachment, neuroscience, sensory processing needs, and relating difficulties that may be experienced after ACEs.” Evidence from Section 8 concluded that “universal attachment literacy across training curricula for all child- and family-facing professions” is essential. Trauma-informed practice: More in-depth and widespread training in trauma-informed practice was recommended by Mellow Parenting, Nurture International, the RCGPS, Stop It Now, and both Jay Haston and Aidan Phillips from lived-experience perspectives. The Scottish Government has established the National Trauma Training Programme, which has trained over 80,000 people by 2025 (Scottish Government, 2025c). However, the evidence suggests a significant implementation gap: while training is available, only around 40% of those trained report sustained changes to their practice (Trauma Framework Evaluation, 2025). This points to the importance of embedding learning through ongoing supervision and support. Relationship skills: The RCGPS highlighted that “health professionals need to model and encourage attunement between parents and children”—suggesting that professional training must include developing professionals’ own relationship and emotional regulation skills. Evidence from Section 8 concluded that “professional competence must include emotional competence. From midwives to teachers to police officers, the capacity to recognise and respond to distress with empathy should be regarded as a core skill.” The Solihull Approach was identified as an effective model for professional training, equipping health visitors, nursery nurses, and other practitioners to use a consistent framework. A key strength is that multi-professional engagement in training allows effective communication between services. 19.7.3 Sector-Specific Training Requirements Evidence across sections identified specific training needs: Health visitors: Better training in overall developmental processes, how early-identified issues predict later problems, how to address early-identified issues, and how to refer families effectively. Training in assessment of parent-child relationships using validated tools.Midwives and maternity services: Enhanced training in mental health assessment, motivational interviewing, trauma-informed care, and brief intervention for substance use. Specialist training in identifying domestic violence during pregnancy. GPs and primary care: Training in family mental health assessment, early intervention, recognising ACEs, and trauma-informed inquiry. Protected Learning Time to embed new practices. Early years practitioners: Rigorous training focused on child development, attachment, play pedagogy, and emotional intelligence. Extended supervised placements and ongoing mentoring. Education staff: Whole-school attachment-informed approaches requiring all staff—not just specialists—to understand attachment, trauma, and relationship-focused practice. South Lanarkshire’s attachment strategy provides a model. Child sexual abuse prevention: Significant investment in professional training to equip practitioners across health, education, police, and social work to identify and respond confidently to CSA. The Lucy Faithfull Foundation recommended specific training modules drawing on the Child Sexual Abuse Practice Leads Programme developed in England and Wales. 19.7.4 Implementation Requirements The evidence was clear that training alone is insufficient. Section 9 noted that “purchasing programmes or distributing materials is insufficient—practitioners need to understand child development, the importance of these skills, and how to support them. They need modelling, coaching, and troubleshooting support. Workforce development is therefore not incidental to programme success but central to it.” Tony McDaid’s experience in South Lanarkshire demonstrated that whole-system transformation is possible: “all members of staff (teachers, cooks, janitors etc.) have all had training” in attachment approaches. But this requires sustained investment over several years to embed practice, not just teach principles. 19.8 Housing 19.8.1 Housing Stress and Child Development Several witnesses identified housing as a critical factor in family stress and child outcomes. Desmond Runyan cited evidence that “a study of a program to support low-income housing was associated with a 4% reduction in child neglect.” Professor Ted Melhuish offered a broader structural critique: “Housing Policy: current housing policies group together disadvantaged families in ghettos of disadvantage. These ghettos establish sub-cultures which promote poor parenting, and increased risk for children of behaviour problems, abuse etc. Our research has found that children growing up in areas with mixed populations do considerably better than equally disadvantaged children in areas which are wholly disadvantaged. It would take a generation to change the impact of past bad mistakes, but the impact over time of a change in Housing policy would be profound.” 19.8.2 Youth Homelessness Evidence on youth homelessness reveals a population at extreme risk, typically with extensive ACE histories. Josh Littlejohn, co-founder of Social Bite in Scotland, described the pattern clearly: “People typically got dealt some really quite harrowing cards when they were born… had typically suffered some really quite traumatic childhood experiences, more often than not, grew up in the care system and quite often became homeless in their late teenage years… it was very systemic, and it seemed that if you were dealt certain cards in life, it was almost your destiny.” The scale remains substantial and has increased since the pandemic. An estimated 121,000 young people aged 18–25 approached councils as homeless in England alone in 2024, up 10% from 2018 figures (Centrepoint, 2025). Scotland saw 32,000 households assessed as homeless in 2024–25, including thousands of young people. The “hidden homeless”—those not claiming government support, often sofa-surfing with friends—may number up to one million UK-wide (Homelessness Monitor England, 2025). The Missing People Organisation estimates that over 140,000 minors go missing annually, many fleeing family breakdown or abuse. Research by Centrepoint (2025) identifies family breakdown as the most common cause, accounting for 40–50% of cases. Many young people flee emotional, physical, or sexual abuse; are rejected after a parent forms a new family; or are pushed out when child benefit ceases at age 16. The link with adverse childhood experiences is stark: research indicates that 70–80% of homeless youth have ACE scores of four or more, compounding risks of mental illness and substance misuse (Bellis et al., 2024). The mental health consequences are severe. Young people living in hostels or bed-and breakfast accommodation are eight times more likely to suffer mental illness than the general population. Those living on the streets are eleven times more likely. 19.8.3 The Housing First Model Finland provides the most compelling evidence for an alternative approach. It remains the only European country to have substantially reduced homelessness, having effectively eliminated street sleeping. The Housing First model is built on a simple principle: people cannot resolve other problems—addiction, mental health, employment—without stable housing first. Finland phased out temporary and night-only shelters, replacing them with sustainable affordable housing. Twenty-four-hour shelters were maintained during the transition period, while registered homeless individuals were placed with friends or family until permanent residences could be found or built. The approach treats housing as a right and foundation, not a reward for compliance with other interventions. By 2024, Finland’s total homelessness had fallen to approximately 3,600—down 50% since 2010—with youth homelessness rates halved through integrated services (Finnish Government, 2025). 19.8.4 Housing First Trials in England The UK Government allocated £28 million to trial Housing First in Liverpool City Region, Greater Manchester, and the West Midlands Combined Authority from 2018. Evaluation of these pilots provides encouraging evidence for the model’s effectiveness. Across the three areas, Housing First housed over 1,100 people by mid-2023. Retention rates were high: 75–90% of participants remained housed after 12–24 months, substantially exceeding outcomes from traditional approaches. Rough sleeping reduced by 20–30% in pilot zones. In Greater Manchester, 80% of participants reported better mental health; Liverpool achieved 90% tenancy sustainment. Improvements were also recorded in health outcomes (fewer hospital admissions) and employment (10–15% entered work or training) (Homeless Link, 2025; Social Market Foundation, 2025). However, progress has stalled since the pilots ended in 2022, with limited national rollout due to funding constraints and housing shortages. Only around 1,000 units were delivered against an estimated need of 16,000. The new UK Government’s National Plan to End Homelessness (December 2025) commits to expanding Housing First with over £100 million investment, emphasising prevention alongside a target of 1.5 million new homes, though implementation remains at an early stage. Wales has strengthened its legislative framework through the Housing (Wales) Act 2014, which introduced a “prevention and relief” duty requiring local authorities to prevent homelessness for all eligible households threatened within 56 days, irrespective of priority need or intentionality. By 2024, this approach had reduced youth homelessness by 15–20% through early intervention, demonstrating the value of prevention-focused legislation (Welsh Government, 2025). 19.8.5 Recommendations Centrepoint’s analysis recommended: Central government should: - Implement a cross-departmental homelessness strategy coordinating action across departments, reflected at local authority level - Conduct a national review of mediation services and efficacy of different approaches, ensuring effective mediation is available in every local authority - Ensure holistic early family support as part of broader child welfare strategy - Introduce a homelessness prevention duty and stronger advice and information duty Local authorities should: - Signpost all young people presenting at housing services to independent advocacy services, irrespective of priority need, intentionality, or local connection - Provide youth-specific emergency and temporary accommodation suitable for young people requiring respite while assessment is undertaken and support put in place -Assess staff turnover in teams working with vulnerable families and implement strategies addressing causes with tangible solutions The economic case for prevention is strong. Centrepoint’s analysis concluded that prevention of youth homelessness would yield a net benefit of over £500 million per annum. Family mediation typically costs £1,000–2,000 per case compared to £20,000 or more for crisis intervention, resolving many problems at a fraction of the cost to the public purse. 19.9 Conclusions and Recommendations The evidence presented to the Commission on providers, professionals, and housing points to several interconnected conclusions. First, Scotland’s universal services provide a strong foundation but require strengthening. The Universal Health Visiting Pathway, expanded early learning and childcare, and investment in whole family support represent significant commitments. However, workforce pressures—inadequate numbers, excessive caseloads, high turnover, role drift, and training gaps—undermine the capacity of these services to deliver relationship-based, preventive support. Second, professional training is both inadequate and insufficiently implemented. Despite the availability of high-quality training through programmes such as the National Trauma Training Programme, the evidence suggests this is not reaching practitioners at the scale required. Training must extend beyond specialist roles to all adults who encounter children and families, and must be embedded through ongoing supervision, coaching, and practice support rather than one-off courses. Third, integrated service delivery produces better outcomes. Full Service Children’s Centres, family hubs, and co-located services enable the collaboration, communication, and continuity that fragmented services cannot achieve. Investment in physical infrastructure and career structures for staff would address turnover and build workforce stability. Fourth, the early years workforce requires transformation. The gap between Nordic standards and Scottish provision in qualifications, pay, status, and turnover is substantial. Play-based kindergarten approaches will not succeed without the workforce capable of delivering them. Fifth, housing is a foundational determinant of family wellbeing. Current housing policies that concentrate disadvantage compound developmental risks. Youth homelessness represents an acute failure of prevention, with profound ACE histories typically preceding loss of housing. Housing First approaches offer an evidence-based alternative.Recommendations The Commission recommends that Scotland strengthen the health visiting workforce through reduced caseloads (maximum 200 children, lower in deprived areas), enhanced training in attachment, infant mental health, and developmental trajectories, and re-establishment of routine liaison with general practice. The Commission recommends that Scotland re-engage general practice with antenatal and preventive child health, including linking child and parental records to identify cumulative risk, Protected Learning Time for trauma-informed practice, and enhanced multi-disciplinary team working in areas of deprivation. The Commission recommends that Scotland transform the early years workforce through raised qualification requirements, enhanced training in child development, attachment, and play pedagogy, improved pay and career pathways, and elevation of professional status to reflect the developmental importance of work with young children. The Commission recommends that Scotland develop Full Service Children’s Centres or integrated family hubs in every community, co-locating health visiting, early years education, family support, and parenting programmes with stable, well-trained staff supported by appropriate career structures. The Commission recommends that all professionals working with children and families receive comprehensive training in attachment, child development, trauma-informed practice, and relationship-based approaches—with training embedded through ongoing supervision, coaching, and reflective practice rather than one-off courses. The Commission recommends that Scotland review housing policy to prevent concentration of disadvantage, adopt Housing First principles for homeless families and young people, and strengthen the homelessness prevention duty with particular attention to young people leaving care or fleeing family breakdown. References Audit Scotland. (2024). Health and social care integration: Update on progress. Audit Scotland. Bellis, M. A., et al. (2024). Adverse childhood experiences and their association with homelessness. Journal of Public Health. British Medical Journal. (2024). Scotland’s health visitor investment is improving child health and easing pressure on services. BMJ, 384, q448. Centrepoint. (2025). Youth Homelessness Statistics and Causes Report. Centrepoint. Centre for Social Justice. (2025). No Place Like Home: Scaling up Housing First in England. Centre for Social Justice.Department for Education. (2021). Study of Early Education and Development (SEED): Impact Study on Early Education Use and Child Outcomes up to Age Seven Years. Department for Education. European Commission/EACEA/Eurydice. (2019). Key data on early childhood education and care in Europe – 2019 edition. Eurydice Report. Publications Office of the European Union. Finnish Government. (2025). Housing First: Finland’s approach to ending homelessness. Ministry of the Environment. Goff, J., Hall, J., Sylva, K., et al. (2013). Evaluation of Children’s Centres in England (ECCE): Strand 3 – Delivery of family services by Children’s Centres. Department for Education. GOV.UK. (2025). A National Plan to End Homelessness. Ministry of Housing, Communities & Local Government. Homeless Link. (2024). Building a case for Housing First: Regional Pilots final evaluation report. Homeless Link. Homelessness Monitor England. (2025). Annual Report. Crisis. Institute of Health Visiting. (2024). State of Health Visiting, UK survey report. Institute of Health Visiting. Melhuish, E. C. (2005). Early impacts of Sure Start Local Programmes on children and families. National Evaluation of Sure Start. Melhuish, E. C., Belsky, J., Leyland, A. H., & Barnes, J. (2008). Effects of fully-established Sure Start Local Programmes on 3-year-old children and their families living in England. The Lancet, 372(9650), 1641–1647. Melhuish, E. C., Belsky, J., MacPherson, K., & Cullis, A. (2010). The quality of group childcare settings used by 3-4 year old children in Sure Start Local Programme areas and the relationship with child outcomes. Department for Education. Melhuish, E., & Hall, D. (2007). The policy background to Sure Start. In J. Belsky, J. Barnes, & E. Melhuish (Eds.), The National Evaluation of Sure Start: Does area-based early intervention work? (pp. 3–21). Policy Press. Missing People. (2025). Annual Missing Persons Statistics. Missing People Organisation. Moss, P. (2014). Transformative change and real utopias in early childhood education: A story of democracy, experimentation and potentiality. Routledge. Nutbrown, C. (2012). Foundations for quality: The independent review of early education and childcare qualifications. Department for Education. Nursing in Practice. (2024). Health visiting services ‘falling off a cliff’, MPs warn. Nursing in Practice. OECD. (2023). Education at a Glance 2023: OECD Indicators. OECD Publishing.OECD. (2025a). TALIS Starting Strong 2024: Supporting Early Childhood Teachers. OECD Publishing. Renfrewshire Health and Social Care Partnership. (2025). Health Visiting Service Report. Renfrewshire HSCP. Scottish Government. (2022). Written submission to the Commission. Scottish Government. Scottish Government. (2023a). Early Learning and Childcare Workforce. Scottish Government. Scottish Government. (2025a). Enhancing delivery of health visiting service: Scotland’s Health Visiting Action Plan 2025–2035. Scottish Government. Scottish Government. (2025b). Early Years Workforce Strategy. Scottish Government. Scottish Government. (2025c). National Trauma Training Programme: Progress Report. Scottish Government. Social Market Foundation. (2023). The economic case for community care. Social Market Foundation. Solihull Approach. (2025). Evaluation of the Solihull Approach in Scottish Settings. Solihull Approach. Trauma Framework Evaluation. (2025). Implementation of Trauma-Informed Practice in Scotland. NHS Education for Scotland. Welsh Government. (2025). Homelessness Prevention: Outcomes Report. Welsh Government.